T-cell acute lymphoblastic leukemia/lymphoma (T-ALL) is a precursor T-cell neoplasm.
What is the Pathology of T-cell Acute Lymphoblastic Leukemia/Lymphoma (T-ALL)?
The pathology of t-cell acute lymphoblastic leukemia/lymphoma is:
-Etiology: The cause of T-cell acute lymphoblastic leukemia/lymphoma is not well characterized.
-Genes involved: HOX 11, CFLAR, NOTCH 2 BTG3 genes.
-Pathogenesis: The sequence of events that lead to T-cell acute lymphoblastic leukemia/lymphoma involves transcriptional deregulation of oncogenes/oncosuppressors, NOTCH 1 signaling, cell cycle deregulation, kinase signaling pathway, epigenetic deregulation ribosomal dysfunction and altered expression of oncogenic miRNAs or long non coding RNA.
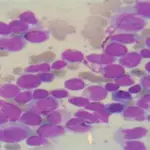
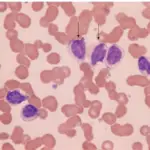
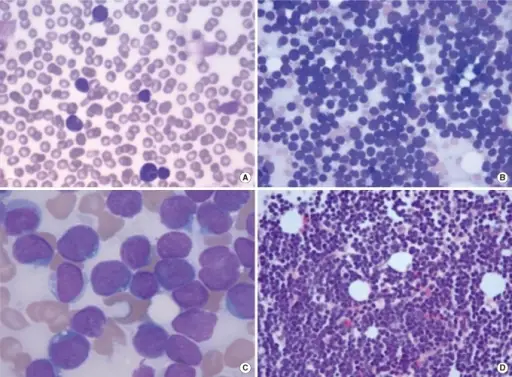
-Histology: The histology associated with t-cell acute lymphoblastic leukemia/lymphoma shows scant cytoplasm, delicate chromatin, indistinct nucleoli, convoluted nuclear membrane and grooves. Frequent mitotic figures and interspersed benign macrophages may be present. Complete architectural effacement or partial involvement with paracortical infiltrate with germinal center sparing of lymph nodes are seen.
 T-cell Acute Lymphoblastic Leukemia. Blasts in the bone marrow smear. T-cell Acute Lymphoblastic Leukemia with del (7) (q11.2q22) and Aberrant Expression of Myeloid Markers. Ahmadzadeh A, Saedi S, Jaseb K, Asnafi AA, Alghasi A, Saki N - International journal of hematology-oncology and stem cell research (2013).
T-cell Acute Lymphoblastic Leukemia. Blasts in the bone marrow smear. T-cell Acute Lymphoblastic Leukemia with del (7) (q11.2q22) and Aberrant Expression of Myeloid Markers. Ahmadzadeh A, Saedi S, Jaseb K, Asnafi AA, Alghasi A, Saki N - International journal of hematology-oncology and stem cell research (2013).
How does T-cell Acute Lymphoblastic Leukemia/Lymphoma (T-ALL) Present?
Patients with T-cell acute lymphoblastic leukemia/lymphoma typically presents in older children with a male predominance. The symptoms, features, and clinical findings associated with (t-cell acute lymphoblastic leukemia/lymphoma are generally non-specific and are mostly due to bone marrow dysfunction. This include weakness, fatigue, shortness of breath, fever, malaise, night sweats, lymphadenopathy, pancytopenia, mucosal bleeding, and purpura.
How is T-cell Acute Lymphoblastic Leukemia/Lymphoma (T-ALL) Diagnosed?
T-cell acute lymphoblastic leukemia/lymphoma (T-ALL) is diagnosed mainly through biopsy of the bone marrow to determine the type of leukemia. Complete blood count and peripheral blood smears (Lymphoblasts of 20% or more of marrow cells) may be helpful.
How is T-cell Acute Lymphoblastic Leukemia/Lymphoma (T-ALL) Treated?
T-cell acute lymphoblastic leukemia/lymphoma (T-ALL) is treated with chemotherapy along with steroids. Stem cell transplant is indicated only in younger patients that do not respond to chemotherapy.
What is the Prognosis of T-cell Acute Lymphoblastic Leukemia/Lymphoma (T-ALL)?
The prognosis of T-cell acute lymphoblastic leukemia/lymphoma is variable depending on the genes involved. HOX11 overexpression in adults indicate good prognosis while expressions of CFLAR, NOTCH 2, and BTG3 genes indicate poor prognosis.