Thyroid gland pathology includes:
- Thyroglossal duct cyst
- Lingual thyroid
- Hyperthyroidism
- Graves’ disease
- Multinodular goiter
- Cretinism
- Myxedema
- Hashimoto thyroiditis
- Subacute granulomatous thyroiditis
- Riedel fibrosing thyroiditis
- Follicular thyroid adenoma
- Follicular thyroid carcinoma
- Papillary thyroid carcinoma
- Medullary thyroid carcinoma
- Anaplastic thyroid carcinoma
Thyroglossal Duct Cyst
Thyroglossal duct cyst is a cystic dilation of thyroglossal duct remnant.
The thyroglossal duct leads from the base of the tongue to the anterior neck, where the thyroid develops.
While the thyroglossal duct ordinarily involutes, a prolonged duct may enlarge cystically.
Thyroglossal duct cyst presents as an anterior neck mass.
 Thyroglossal Duct Cyst. Ultrasound image of thyroglossal duct cyst. Nevit Dilmen. Not altered. CC BY-SA 3.0
Thyroglossal Duct Cyst. Ultrasound image of thyroglossal duct cyst. Nevit Dilmen. Not altered. CC BY-SA 3.0





Lingual Thyroid
The presence of thyroid tissue at the base of the tongue is known as lingual thyroid.
Lingual thyroid appears as a mass of tongue at the base.
 Lingual Thyroid. For context, see Computed tomography of the thyroid. Mnahi Bin Saeedan, Ibtisam Musallam Aljohani, Ayman Omar Khushaim, Salwa Qasim Bukhari, and Salahudin Tayeb Elnaas - (2016). "Thyroid computed tomography imaging: pictorial review of variable pathologies". Insights into Imaging 7 (4): 601–617. DOI:10.1007/s13244-016-0506-5. ISSN 1869-4101.. Not altered. CC BY 4.0
Lingual Thyroid. For context, see Computed tomography of the thyroid. Mnahi Bin Saeedan, Ibtisam Musallam Aljohani, Ayman Omar Khushaim, Salwa Qasim Bukhari, and Salahudin Tayeb Elnaas - (2016). "Thyroid computed tomography imaging: pictorial review of variable pathologies". Insights into Imaging 7 (4): 601–617. DOI:10.1007/s13244-016-0506-5. ISSN 1869-4101.. Not altered. CC BY 4.0
Hyperthyroidism
When the thyroid gland overproduces the hormone thyroxine, hyperthyroidism (overactive thyroid) occurs.
Hyperthyroidism causes an increase in sympathetic nervous system activity and a rise in basal metabolic rate as a result of increased Na+-K+ ATPase production and B1-adrenergic receptor expression, respectively.
Symptoms of hyperthyroidism include:
- Weight loss despite increased appetite
- Heat intolerance
- Sweating
- Tachycardia
- Tremor
- Anxiety
 Graves Disease. Histopathological image of diffuse hyperplasia of the thyroid gland clinically presenting as hyperthyroidism. Not altered. CC BY-SA 3.0
Graves Disease. Histopathological image of diffuse hyperplasia of the thyroid gland clinically presenting as hyperthyroidism. Not altered. CC BY-SA 3.0






Graves’ Disease
Graves’ disease is an autoimmune disorder that affects the thyroid.
In Graves’ disease, autoantibody IgG activates the thyroid stimulating hormone (TSH) receptor which increases thyroid hormone production and release.
In women of childbearing age (between the ages of 20-years-old and 40-years-old) this condition is the most common cause of hyperthyroidism.
Hyperthyroidism, diffuse goiter, and persistent thyroid stimulating hormone (TSH) stimulation cause thyroid hyperplasia and hypertrophy as clinical characteristics.
Clinical features of Graves’ disease include:
- Exophthalmos aka proptosis
- Pretibial myxedema may occur as well
Thyroid stimulating hormone (TSH) activation causes glycosaminoglycan buildup, including chondroitin sulfate and hyaluronic acid, as well as inflammation, fibrosis, and edema, which result in exophthalmos and pretibial myxedema.
Fibroblasts behind the orbit and atop the shin express the thyroid stimulating hormone (TSH) receptor.
Histology of Graves’ disease shows irregular follicles with scalloped colloids and chronic inflammation are seen in histology.
Laboratory findings of Graves’ disease show:
- Increased total and free T4
- Decreased thyroid stimulating hormone (TSH)
- Hypocholesterolemia
- Elevated blood glucose
Free T4 downregulates thyrotropin-releasing hormone (TRH) receptors in the anterior pituitary to reduce thyroid stimulating hormone (TSH) release.
Treatment of Graves disease includes thioamide and radioiodine ablation.
Thyroid storm is a potentially fatal condition caused by huge hormone excess and high catecholamines, which are typically produced in reaction to stressors like surgery or delivery.
The symptoms of thyroid storm include:
- Hypovolemic shock
- Tachycardia
- Heat intolerance
- Vomiting
Beta-blockers, steroids, and propylthiouracil (PTU) are potential treatment options.
Propylthiouracil (PTU) prevents peripheral T4 to T3 conversion as well as the peroxidase-mediated oxidation, organification, and coupling phases of thyroid hormone production.
 Graves Disease. Scan of affected thyroid before (top) and after (bottom) radioiodine therapy MBq. Not altered. Copyrighted free use
Graves Disease. Scan of affected thyroid before (top) and after (bottom) radioiodine therapy MBq. Not altered. Copyrighted free use




Multinodular Goiter
Multinodular goiter is described as numerous nodules in an enlarged thyroid gland caused by a relative iodine deficit.
Multinodular goiters are typically nontoxic (euthyroid).
Rarely, an area will lose its thyroid stimulating hormone (TSH)-dependent state, causing T1 release, hyperthyroidism, or toxic goiter.
 Multinodular Goiter. Goitre with toxic adenoma Drahreg. Not altered. CC BY-SA 3.0
Multinodular Goiter. Goitre with toxic adenoma Drahreg. Not altered. CC BY-SA 3.0




Hypothyroidism
Cretinism
Hypothyroidism in newborns may result in cretinism.
Symptoms of cretinism include:
- Mental retardation
- Oversized tongue
- Small stature
- Macroglossia (enlarged tongue)
- Skeletal deformities
- Coarse facial characteristics
Thyroid hormone is required for normal brain and skeletal development.
Cretinism may be caused by:
- Maternal hypothyroidism during early pregnancy
- Thyroid agenesis
- Dyshormonogenetic goiter
- Iodine deficiency
 Cretinism. Ultrasonography of cervical region. In this case, the thyroid gland (arrowsindicating the right and left lobes) presents with much reduced dimensions and increased echogenicity. Sonographic evaluation of children with congenital hypothyroidism: Sedassari Ade A, de Souza LR, Sedassari Nde A, Borges Mde F, Palhares HM, de Andrade Neto GB - Radiologia brasileira (2015 Jul-Aug). Not Altered. CC.
Cretinism. Ultrasonography of cervical region. In this case, the thyroid gland (arrowsindicating the right and left lobes) presents with much reduced dimensions and increased echogenicity. Sonographic evaluation of children with congenital hypothyroidism: Sedassari Ade A, de Souza LR, Sedassari Nde A, Borges Mde F, Palhares HM, de Andrade Neto GB - Radiologia brasileira (2015 Jul-Aug). Not Altered. CC.
Myxedema
Older children or adults with myxedema have hypothyroidism, which is characterized by a decline in basal metabolic rate and a reduction in sympathetic nervous system activity.
Myxedema is the accumulation of glycosaminoglycans in the skin and soft tissue, which causes weight gain despite a normal appetite and a slowing of mental activity.
Myxedema also causes a deepening of voice and tongue enlargement.
Myxedema also results in muscle weakness, cold sensitivity with decreased sweating, bradycardia with decreased cardiac output, weariness, oligomenorrhea, hypercholesterolemia, and constipation.
Causes of myxedema include:
- Iodine deficiency
- Hashimoto thyroiditis
- Lithium medication use
- Surgical removal of the thyroid
- Radioactive ablation of the thyroid
 Myxedema. Woman with myxedema, Bulgaria, 1930s. Unknown author - Not altered.. Public domain.
Myxedema. Woman with myxedema, Bulgaria, 1930s. Unknown author - Not altered.. Public domain.


Thyroiditis
Hashimoto Thyroiditis
Hashimoto thyroiditis is the HLA-DRS-related autoimmune destruction of the thyroid gland.
The most frequent reason for hypothyroidism in areas with sufficient iodine levels.
The progression from hyperthyroidism to hypothyroidism may begin out as follicular damage-induced hyperthyroidism.
The presence of antithyroglobulin and antimicrosomal antibodies is frequently indicative of thyroid impairment.
Histologically, Hashimoto thyroiditis shows chronic inflammation with germinal centers and Hürthle cells is associated with eosinophilic metaplasia of cells lining follicles.
There is an elevated risk for B-cell lymphoma in Hashimoto thyroiditis.
 Hashimoto Thyroiditis. Ultrasound imaging of the thyroid gland (right lobe longitudinal) in a person with Hashimoto thyroiditis Drahreg01. Not altered. CC BY-SA 3.0
Hashimoto Thyroiditis. Ultrasound imaging of the thyroid gland (right lobe longitudinal) in a person with Hashimoto thyroiditis Drahreg01. Not altered. CC BY-SA 3.0


Subacute Granulomatous (De Quervain) Thyroiditis
Subacute granulomatous thyroiditis is due to a viral infection that manifests as a sensitive thyroid and temporary hyperthyroidism.
Subacute granulomatous thyroiditis is also called de Quervain thyroiditis.
Subacute granulomatous thyroiditis is self-limited and does not progress to hypothyroidism.
 Thyroiditis") Subacute Granulomatous (De Quervain) Thyroiditis. Intermediate magnification micrograph of subacute thyroiditis, also known as idiopathic granulomatous thyroiditis. H&E stain. Related images Intermed. mag. High mag. Very high mag. Nephron -Not altered. CC BY-SA 3.0
Subacute Granulomatous (De Quervain) Thyroiditis. Intermediate magnification micrograph of subacute thyroiditis, also known as idiopathic granulomatous thyroiditis. H&E stain. Related images Intermed. mag. High mag. Very high mag. Nephron -Not altered. CC BY-SA 3.0
Riedel Fibrosing Thyroiditis
Riedel fibrosing thyroiditis manifests as hypothyroidism with a “hard as wood,” non-tender thyroid gland and is a chronic inflammation with significant thyroid fibrosis.
Local structures like the airway may get affected by a fibrosis that has spread.
Clinically, Riedel fibrosing thyroiditis resembles anaplastic carcinoma, but the patients are younger, no malignant cells are present.
Thyroid Neoplasia
Thyroid nodules are more likely to be benign than malignant, and thyroid neoplasia usually appears as a distinct, solitary nodule.
I-131 radioactive uptake studies are useful to further characterize nodules.
Increased uptake (hot nodule) is seen in Graves’ disease or nodular goiter.
Decreased uptake (cold nodule) is seen in adenoma and carcinoma and they often warrant biopsy.
Biopsy is performed by fine needle aspiration (FNA).
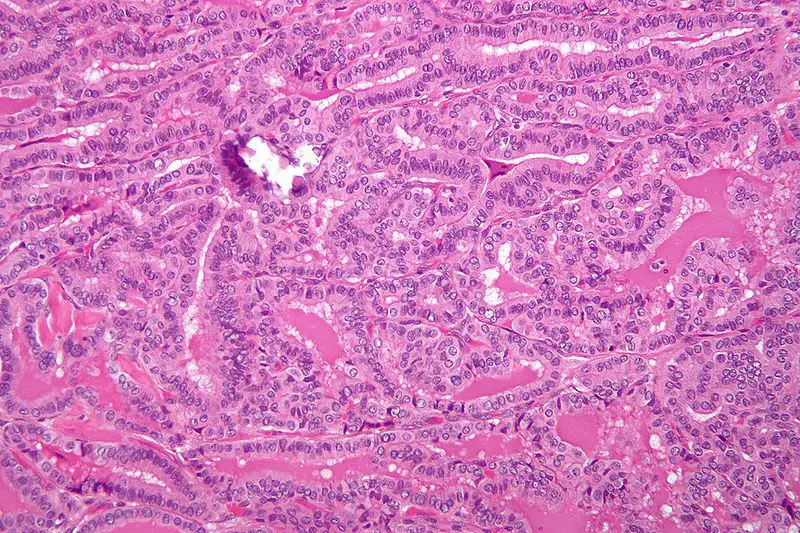
 Papillary Thyroid Carcinoma. Histopatholgical image of papillary carcinoma of the thyroid gland obtained by a total thyroidectomy. Hematoxylin and eosin stain. KGH. Not altered. CC BY-SA 3.0
Papillary Thyroid Carcinoma. Histopatholgical image of papillary carcinoma of the thyroid gland obtained by a total thyroidectomy. Hematoxylin and eosin stain. KGH. Not altered. CC BY-SA 3.0

Follicular Thyroid Adenoma
Follicular thyroid adenoma is characterized by a benign proliferation of follicles encased in an inactive fibrous capsule.
Follicular thyroid adenoma does not invade the capsule.
 Follicular Adenomas. (a) Photomicrograph of a follicular adenoma (hematoxylineosin, ×LP) (b) A follicular adenoma, immunostaining for cytokeratin 19, focal positive (1+) (IHC, ×LP). Cytokeratin 19 immunoreactivity in the diagnosis of papillary thyroid carcinoma: Bose D, Das RN, Chatterjee U, Banerjee U - Indian journal of medical and paediatric oncology : official journal of Indian Society of Medical & Paediatric Oncology (2012). Not Altered. CC.
Follicular Adenomas. (a) Photomicrograph of a follicular adenoma (hematoxylineosin, ×LP) (b) A follicular adenoma, immunostaining for cytokeratin 19, focal positive (1+) (IHC, ×LP). Cytokeratin 19 immunoreactivity in the diagnosis of papillary thyroid carcinoma: Bose D, Das RN, Chatterjee U, Banerjee U - Indian journal of medical and paediatric oncology : official journal of Indian Society of Medical & Paediatric Oncology (2012). Not Altered. CC.

Follicular Thyroid Carcinoma
Follicular thyroid carcinoma (FTC) is the malignant proliferation of thyroid follicles with invasion through the capsule.
Follicular thyroid carcinoma invades the capsule.
The distinction between a follicular adenoma and a follicular carcinoma cannot be made by fine needle aspiration (FNA) because FNA only looks at the cells and not the entire capsule under a microscope.
Metastasis of papillary thyroid carcinoma (PTC) generally occurs via hematogenous spread.
 Follicular Thyroid Carcinoma. Follicular thyroid carcinoma, abbreviated FTC, is a type of thyroid cancer. H&E stain. Nephron. Not altered. CC BY-SA 4.0
Follicular Thyroid Carcinoma. Follicular thyroid carcinoma, abbreviated FTC, is a type of thyroid cancer. H&E stain. Nephron. Not altered. CC BY-SA 4.0

Papillary Thyroid Carcinoma
Papillary thyroid carcinoma (PTC) is the most common kind of thyroid cancer.
A significant risk factor for papillary thyroid carcinoma (PTC) is early ionizing radiation exposure.
Histology of papillary thyroid carcinoma (PTC) shows papillae that are lined by cells with Orphan Annie eye nuclei that are clear and nuclear grooves that are frequently found around psammoma bodies.
The prognosis of papillary thyroid carcinoma (PTC) is excellent.
The 10-year survival rate of papillary thyroid carcinoma (PTC) is greater than 95% despite the fact that this frequently spreads to cervical or neck lymph nodes.
 Papillary Thyroid Carcinoma. Micrograph of papillary thyroid carcinoma, tall cell variant - high magnification. H&E stain. Nephron. CC BY-SA 3.0
Papillary Thyroid Carcinoma. Micrograph of papillary thyroid carcinoma, tall cell variant - high magnification. H&E stain. Nephron. CC BY-SA 3.0







Medullary Thyroid Carcinoma
The malignant proliferation of parafollicular C cells, which makes up 5% of thyroid carcinomas, is known as medullary thyroid carcinoma.
Medullary thyroid carcinoma may result in high quantities of calcitonin and cause hypocalcemia.
Histology of medullary thyroid carcinoma reveals sheets of malignant cells in a calcitonin derived amyloid stroma.
Multiple endocrine neoplasia (MEN) 2A and 2B, which are linked to mutations in the RET oncogene, are often the cause of familial cases of medullary thyroid carcinoma.
When the RET mutation is found, a prophylactic thyroidectomy is necessary.
 Clinical and histological presentation of FMTC/CAA–D. Macular amyloidosis: brown hyperpigmented macules on the upper back, shoulders, arms, and legs. (A) Postoperative neck scar and brown hyperpigmented macular skin lesion on the arms (individual II-5). (B–D) Macular amyloidosis: macules showing pigmentation with a rippled or reticulated pattern and with scabby scratches on the upper back and extremities (individual III-3). E. Lichen amyloidosis: dry, scaly, and thickened SKIN with hyperpigmentation and remnant white patches on the lower leg (individual II-5). F. Close-up of lichen amyloidosis: multiple monomorphic skin-colored and clustered lichenified papules with white thin scales on the lower leg (individual II-5). G. Small hyaline deposits of amyloid were situated in the papillary dermis. There is overlying epidermal hyperplasia (hematoxylin & eosin; original magnification, × 100). H. Globular deposits of amyloid were positive for crystal violet staining (original magnification, × 200). I. The papillary dermal deposits were positive for Congo red stain (original magnification, × 400). RET mutation p.S891A in a Chinese family with familial medullary thyroid carcinoma and associated cutaneous amyloidosis binding OSMR variant p.G513D. Qi XP, Zhao JQ, Chen ZG, Cao JL, Du J, Liu NF, Li F, Sheng M, Fu E, Guo J, Jia H, Zhang YM, Ma JM - Oncotarget (2015). Not Altered. CC.
Clinical and histological presentation of FMTC/CAA–D. Macular amyloidosis: brown hyperpigmented macules on the upper back, shoulders, arms, and legs. (A) Postoperative neck scar and brown hyperpigmented macular skin lesion on the arms (individual II-5). (B–D) Macular amyloidosis: macules showing pigmentation with a rippled or reticulated pattern and with scabby scratches on the upper back and extremities (individual III-3). E. Lichen amyloidosis: dry, scaly, and thickened SKIN with hyperpigmentation and remnant white patches on the lower leg (individual II-5). F. Close-up of lichen amyloidosis: multiple monomorphic skin-colored and clustered lichenified papules with white thin scales on the lower leg (individual II-5). G. Small hyaline deposits of amyloid were situated in the papillary dermis. There is overlying epidermal hyperplasia (hematoxylin & eosin; original magnification, × 100). H. Globular deposits of amyloid were positive for crystal violet staining (original magnification, × 200). I. The papillary dermal deposits were positive for Congo red stain (original magnification, × 400). RET mutation p.S891A in a Chinese family with familial medullary thyroid carcinoma and associated cutaneous amyloidosis binding OSMR variant p.G513D. Qi XP, Zhao JQ, Chen ZG, Cao JL, Du J, Liu NF, Li F, Sheng M, Fu E, Guo J, Jia H, Zhang YM, Ma JM - Oncotarget (2015). Not Altered. CC.


Anaplastic Thyroid Carcinoma
An undifferentiated malignant thyroid tumor called anaplastic carcinoma is typically detected in older people.
Anaplastic carcinoma frequently infiltrates nearby structures, causing dysphagia or respiratory problems.
Anaplastic carcinoma has a poor prognosis.
 Thyroid Carcinomas. (A, B) Papillary thyroid carcinoma at 23 years of age. (C, D) Recurrent papillary thyroid carcinoma after 5 years. Poorly differentiated cells are seen at focal areas of the papillary thyroid carcinoma. (E, F) Recurrent anaplastic thyroid carcinoma in the pretrachea adjacent thyroid bed. Anaplastic Transformation of Papillary Thyroid Carcinoma in a Young Man: A Case Study with Immunohistochemical and BRAF Analysis: Park JH, Kwon HJ, Park CS, Hong S - Korean journal of pathology (2014). Not Altered. CC.
Thyroid Carcinomas. (A, B) Papillary thyroid carcinoma at 23 years of age. (C, D) Recurrent papillary thyroid carcinoma after 5 years. Poorly differentiated cells are seen at focal areas of the papillary thyroid carcinoma. (E, F) Recurrent anaplastic thyroid carcinoma in the pretrachea adjacent thyroid bed. Anaplastic Transformation of Papillary Thyroid Carcinoma in a Young Man: A Case Study with Immunohistochemical and BRAF Analysis: Park JH, Kwon HJ, Park CS, Hong S - Korean journal of pathology (2014). Not Altered. CC.