Myeloproliferative Disorders
Myeloproliferative Disorders Pathology Video
Myeloproliferative disorders are neoplastic proliferation of myeloid cells.
Myeloproliferative disorders typically occur in late adulthood (average age is 55-years-old).
Myeloproliferative disorders are associated with:
- Leukocytosis (high white blood cell count)
- Hypercellular bone marrow
In myeloproliferative disorders there is an increase in all the cells of myeloid lineage.
Myeloproliferative disorders are categorized based on the dominant myeloid cell that is produced.
Complications include of myeloproliferative disorders include:
- High risk of hyperuricemia and gout because of turnover of cells
- Transition into acute leukemia or progression to marrow fibrosis
 Myeloproliferative Disorders. Myelogram of someone with a myeloproliferative disorder. Elm'hadi C1,2, Khmamouche MR3, Tanz R3, Toreis M3, Mahtat E4, Allaoui M5, Oukabli M5, Messaoudi N6, Errihani H7, Ichou M3. Not altered. CC BY 4.0
Myeloproliferative Disorders. Myelogram of someone with a myeloproliferative disorder. Elm'hadi C1,2, Khmamouche MR3, Tanz R3, Toreis M3, Mahtat E4, Allaoui M5, Oukabli M5, Messaoudi N6, Errihani H7, Ichou M3. Not altered. CC BY 4.0
Chronic Myeloid Leukemia (CML)
Chronic myeloid leukemia is due to neoplastic proliferation of mature myeloid cells, in particular, granulocytes and granulocyte precursors.
An increase of basophils is characteristic of chronic myeloid leukemia (CML).
Chronic myeloid leukemia is typically driven by the Philadelphia chromosome t(9;22), which results in the production of a BCR-ABL fusion protein with higher tyrosine kinase activity.
Imatinib, which inhibits tyrosine kinase activity, is the first line of treatment of chronic myeloid leukemia.
Splenomegaly is common in chronic myeloid leukemia.
Spleen enlargement indicates an accelerated phase of disease.
Acute leukemia transformation typically occurs shortly after.
Due to a mutation in a pluripotent stem cell, chronic myeloid leukemia can progress:
- Acute myeloid leukemia (AML) (2/3 of cases)
- Acute lymphoblastic leukemia (ALL) (1/3 of cases)
Leukocyte alkaline phosphatase (LAP) staining distinguishes chronic myeloid leukemia (CML) from a leukemoid reaction.
Leukocyte alkaline phosphatase (LAP) is negative in chronic myeloid leukemia (CML).
Leukocyte alkaline phosphatase (LAP) is positive in leukemoid reactions, such as reactive neutrophilic leukocytosis.
The granulocytes in a leukemoid reactions are what cause the leukocyte alkaline phosphatase (LAP) positivity.
 Chronic Myeloid Leukemia. Peripheral blood (MGG stain): marked leukocytosis with granulocyte left shift Paulo Henrique Orlandi Mourao - Not altered. CC BY-SA 3.0
Chronic Myeloid Leukemia. Peripheral blood (MGG stain): marked leukocytosis with granulocyte left shift Paulo Henrique Orlandi Mourao - Not altered. CC BY-SA 3.0



Polycythemia Vera (PV)
Polycythemia vera (PV) is due to the neoplastic proliferation of mature myeloid cells, particularly red blood cells.
In polycythemia vera (PV) granulocytes and platelets are typically increased.
Polycythemia vera is related to JAK2 kinase mutation.
Many clinical symptoms of polycythemia vera (PV) are associated with viscous blood.
Symptoms of polycythemia vera (PV) include:
- Blurry vision
- Headache
- High risk of venous thrombosis
- Flushed face because of congestion (plethora)
- Itching, particularly after a bath or shower (because of histamine release from mast cells)
Treatment of polycythemia vera (PV) includes:
- Phlebotomy (first line)
- Hydroxyurea (second line)
Without medical intervention, polycythemia vera (PV) typically results in death within two years.
Reactive polycythemia must be distinguished from polycythemia vera (PV).
In polycythemia vera (PV):
- SaO2 is normal
- Erythropoietin (EPO) levels are low
In reactive polycythemia (PV):
- SaO2 is low
- EPO is elevated
Reactive polycythemia is brought on by:
- Lung illness
- Sleep apnea
- High altitude exposure
- Renal disease
Reactive polycythemia with elevated erythropoietin (EPO) and normal SaO2 levels are typically caused by ectopic renal cell carcinoma production of EPO.
 Polycythemia Vera. BONE MARROW: POLYCYTHEMIA VERA: MYELOID METAPLASIA PHASE Blood smear from a 68-year-old woman with a 13-year history of polycythemia vera treated with phlebotomy, 32-P, and hydroxyurea. There was a 6-to 7-month history of decreasing hemoglobin level and platelet count. There are three red blood cell precursors present and slight to moderate anisopoikilocytosis. (Wright-Giemsa stain) The Armed Forces Institute of Pathology (AFIP) - PEIR Digital Library (Pathology image database). Image# 404905.. Not altered. Public Domain
Polycythemia Vera. BONE MARROW: POLYCYTHEMIA VERA: MYELOID METAPLASIA PHASE Blood smear from a 68-year-old woman with a 13-year history of polycythemia vera treated with phlebotomy, 32-P, and hydroxyurea. There was a 6-to 7-month history of decreasing hemoglobin level and platelet count. There are three red blood cell precursors present and slight to moderate anisopoikilocytosis. (Wright-Giemsa stain) The Armed Forces Institute of Pathology (AFIP) - PEIR Digital Library (Pathology image database). Image# 404905.. Not altered. Public Domain




Essential Thrombocythemia (ET)
Essential thrombocythemia (ET) is due to the neoplastic proliferation of mature myeloid cells, in particular, platelets.
Red blood cells and granulocytes are also raised in essential thrombocythemia (ET).
Essential thrombocythemia (ET) is typically due to a JAK2 kinase mutation.
Symptoms of essential thrombocythemia (ET) are related excess abnormal platelets.
There is a high risk of bleeding and/or thrombosis in essential thrombocythemia (ET).
In rare cases essential thrombocythemia (ET) may advance to marrow fibrosis or acute leukemia.
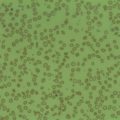
 Essential Thrombocythemia. Histopathological image representing a bone marrow aspirate in a patient with essential thrombocythemia. Hematoxylin & eosin stain. KGH. Not altered. CC.
Essential Thrombocythemia. Histopathological image representing a bone marrow aspirate in a patient with essential thrombocythemia. Hematoxylin & eosin stain. KGH. Not altered. CC.

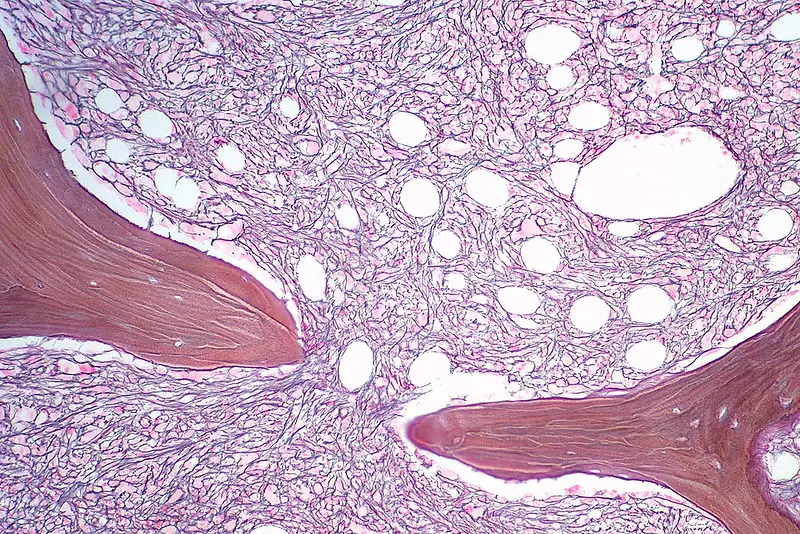
Myelofibrosis
Myelofibrosis is due to the neoplastic proliferation of mature myeloid cells, in particular, megakaryocytes.
Myelofibrosis is related to JAK2 kinase mutation in 50 percent of cases.
Platelet-derived growth factor (PDGF), which megakaryocytes overproduce, causes marrow fibrosis.
In myelofibrosis, splenomegaly occurs due to extra-medullary hematopoiesis.
Histology of myelofibrosis is characterized by:
- A leukoerythroblastic smear with tear-drop red blood cells
- Nucleated red blood cells
- Immature granulocytes
Patients with myelofibrosis have an increased risk of infection, thrombosis, and bleeding.
 Primary Myelofibrosis. An image from a peripheral blood smear showing tears, elliptocytes, schistocytes, and a giant platelet seen in primary myelofibrosis. 50x oil immersion. Michelle To, Valentin Villatoro. From MLS Collection, University of Alberta, https://doi.org/10.7939/R3CJ88201. Not altered. CC.
Primary Myelofibrosis. An image from a peripheral blood smear showing tears, elliptocytes, schistocytes, and a giant platelet seen in primary myelofibrosis. 50x oil immersion. Michelle To, Valentin Villatoro. From MLS Collection, University of Alberta, https://doi.org/10.7939/R3CJ88201. Not altered. CC.