Macrocytic Anemia
Macrocytic Anemia Pathology Video
Macrocytic anemia is anemia with MCV > 100 micrometer3.
Macrocytic anemia is usually caused by folate or vitamin B12 deficiency (megaloblastic anemia).
Folate and vitamin B12 are required for synthesis of DNA precursors.
Folate circulates as methyltetrahydrofolate (methyl THF) in the serum.
The participation in the synthesis of DNA precursors is made possible by the removal of the methyl group.
Transfer of the methyl group to vitamin B12 (cobalamin) occurs under normal circumstances.
The subsequent conversion to homocysteine by vitamin B12 results in methionine.
The synthesis of DNA precursors is impaired by a lack of folate or vitamin B12.
Megaloblastic anemia is caused by abnormal red blood cell (RBC) precursor growth and cell division.
Hypersegmented neutrophils result from granulocytic progenitors that fail to divide properly.
Megaloblastic change can also be detected in rapidly dividing epithelial cells, such as those in the intestine.
Causes of macrocytic anemia include:
- Vitamin B12 deficiency
- Folate deficiency
- Certain drugs (e.g. 5-fluorouracil (5-FU))
- Liver illness
- Alcoholism
 Vitamin B12 Deficiency. Cervical spinal cord MRI in a 49-year-old male presenting with subacute combined degeneration due to a deficit of B12. (A) The midsagittal T2 weighted image shows linear hyperintensity in the posterior portion of the cervical tract of the spinal cord (black arrows). (B) Axial T2 weighted images reveal the selective involvement of the posterior columns. Chiara Briani, Chiara Dalla Torre,1 Valentina Citton,2 Renzo Manara,2,3 Sara Pompanin,1 Gianni Binotto,4 and Fausto Adami4. Not altered. CC BY-SA 3.0
Vitamin B12 Deficiency. Cervical spinal cord MRI in a 49-year-old male presenting with subacute combined degeneration due to a deficit of B12. (A) The midsagittal T2 weighted image shows linear hyperintensity in the posterior portion of the cervical tract of the spinal cord (black arrows). (B) Axial T2 weighted images reveal the selective involvement of the posterior columns. Chiara Briani, Chiara Dalla Torre,1 Valentina Citton,2 Renzo Manara,2,3 Sara Pompanin,1 Gianni Binotto,4 and Fausto Adami4. Not altered. CC BY-SA 3.0


Folate Deficiency
Folate deficiency refers to a lack of homeostatic levels of folate.
Green vegetables and some fruits provide dietary folate.
Folate deficiency develops within months.
Folate is absorbed in the jejunum due to low body storage.
Causes of folate deficiency include:
- Poor diet (e.g., in alcoholics and the elderly)
- Increased demand (e.g., in pregnancy, cancer, and hemolytic anemia)
- Folate antagonist medications such as methotrexate, which inhibits dihydrofolate reductase
Clinical and laboratory findings of folate deficiency include:
- Macrocytic red blood cells and hypersegmented neutrophils (more than 5 lobes)
- Glossitis (inflammation of the tongue)
- Low serum folate
- increased serum homocysteine (which increases the risk thrombosis)
- Normal levels of methyl malonic acid
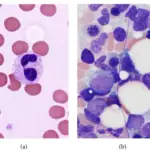
 Anemia of Folate Deficiency. Bone marrow aspirate smear demonstrates numerous megaloblasts and giant metamyelocytes (Wright-Giemsa, ×1000). Pyrexia in a patient with megaloblastic anemia: a case report and literature review. Manuel K, Padhi S, G'boy Varghese R - Iranian journal of medical sciences (2013). Not Altered. CC.
Anemia of Folate Deficiency. Bone marrow aspirate smear demonstrates numerous megaloblasts and giant metamyelocytes (Wright-Giemsa, ×1000). Pyrexia in a patient with megaloblastic anemia: a case report and literature review. Manuel K, Padhi S, G'boy Varghese R - Iranian journal of medical sciences (2013). Not Altered. CC.
Vitamin B12 Deficiency
Vitamin B12 deficiency refers to a lack of homeostatic levels of vitamin B12.
Proteins obtained from animals are complexed with dietary vitamin B12.
Vitamin B12 is released by salivary gland enzymes such as amylase and then bound by R-binder, another salivary gland enzyme, and passed via the stomach.
Vitamin B12 is released from R-binder in the duodenum by pancreatic proteases.
In the small intestine, vitamin B12 binds an intrinsic factor that is produced by gastric parietal cells.
The ileum is where the intrinsic factor-vitamin B12 complex is absorbed.
Due to high hepatic stores of vitamin B12, vitamin B12 deficiency is less prevalent than folate shortage and takes years to develop.
Causes of vitamin B12 deficiency include:
- Pernicious anemia
- Veganism
- Pancreatic insufficiency
- Terminal ileum damage
Pernicious anemia is the most typical cause of a vitamin B12 deficiency.
Intrinsic factor deficiency results from the autoimmune loss of parietal cells in the stomach’s body.
Damage to the terminal ileum and pancreatic insufficiency are two additional factors that contribute to vitamin B12 deficiency (e.g. Crohn disease or Diphyllobothrium latum [fish tapeworm]).
Except in vegetarians, dietary deficiencies of vitamin B12 are uncommon.
Clinical and laboratory findings of vitamin B12 deficiency include:
- Macrocytic red blood cells
- Hypersegmented neutrophils
- Glossitis
- Subacute combined degeneration of the spinal cord
Methylmalonic acid is converted to succinyl CoA with the help of vitamin B12 (which is important in fatty acid metabolism).
Vitamin B12 deficiency results in increased levels of methyl malonic acid, which impairs spinal cord myelination.
Myelination damage leads to:
- Impaired vibratory feeling in the posterior column
- Spastic paresis
- Poor proprioception (lateral corticospinal tract)
Treatment of vitamin B12 is vitamin B12.
- Vitamin B12 Deficiency. Cervical spinal cord MRI in a 49-year-old male presenting with subacute combined degeneration due to a deficit of B12. (A) The midsagittal T2 weighted image shows linear hyperintensity in the posterior portion of the cervical tract of the spinal cord (black arrows). (B) Axial T2 weighted images reveal the selective involvement of the posterior columns. Chiara Briani, Chiara Dalla Torre,1 Valentina Citton,2 Renzo Manara,2,3 Sara Pompanin,1 Gianni Binotto,4 and Fausto Adami4. Not altered. CC BY-SA 3.0