Acute Renal Failure Pathology Video
Acute Renal Failure (ARF)
Acute renal failure (ARF) is the acute, severe decrease in renal function that develops within days.
The hallmark of acute renal failure (ARF) is azotemia, excessive amounts of blood urea nitrogen (BUN) and creatinine in the blood, often with oliguria.
The etiology of acute renal failure is divided into:
- Prerenal azotemia
- Postrenal azotemia
- Intrarenal azotemia
 Acute Renal Failure. Kidney showing marked pallor of the cortex, contrasting to the darker areas of surviving medullary tissue. Haymanj - Not altered. Public Domain
Acute Renal Failure. Kidney showing marked pallor of the cortex, contrasting to the darker areas of surviving medullary tissue. Haymanj - Not altered. Public Domain



Prerenal Azotemia
Prerenal azotemia is caused by renal failure (ARF) and decreased blood supply to the kidneys.
Prerenal azotemia frequently leads to acute renal failure (ARF) and is considered as the common cause.
Reduced blood flow causes oliguria, azotemia, and increase in glomerular filtration rate (GFR).
Reabsorption of fluid and blood urine nitrogen (BUN) ensures that serum BUN:Creatinine ratio is greater than 15 and that tubular function remains intact (fractional excretion of sodium FENa) is less than 1% and urine osmolality (osm) is greater than 500 mOsm/kg.
Postrenal Azotemia
Postrenal azotemia occurs when there is a restriction in the urine’s flow.
Postrenal azotemia is seen in cases of:
- Neurogenic bladder
- Prostatic hypertrophy
- Bladder neck blockage from cancer
- Posterior urethral valves
- Retroperitoneal fibrosis
- Bilateral ureteral obstruction from tumors or stones
Decreased outflow results in decreased glomerular filtration rate (GFR), azotemia, and oliguria.
During the early stage of obstruction there is increased tubular pressure.
The increased tubular pressure forces blood urea nitrogen (BUN) into the blood with serum BUN:Creatinine ratio having greater than 15 and its tubular function remains intact (FENa < 1% and urine osm > 500 mOsm/kg).
With long-standing obstruction, tubular damage ensues, resulting in decreased reabsorption of blood urea nitrogen (BUN) (serum BUN:Cr ratio < 15), decreased reabsorption of sodium (FENa > 2%), and inability to concentrate urine (urine osm < 500 mOsm/kg).
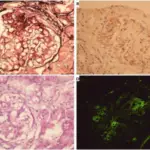
 Acute Antibody Mediated Rejection. A) A 4-year-old child who had good allograft function initially and then developed acute antibody-mediated rejection 2 weeks after deceased donor kidney transplantation. Renal biopsy reveals marked acute tubular necrosis and interstitial hemorrhage. There is evidence of glomerulitis and tubulitis (H&E, 40×). B) Immunofluorescence in this patient reveals diffuse C4d staining of the peritubular capillaries, supporting the diagnosis of acute antibody-mediated rejection. Not Altered. CC. Issues in solid-organ transplantation in children: translational research from bench to bedside. Lipshultz SE, Chandar JJ, Rusconi PG, Fornoni A, Abitbol CL, Burke GW, Zilleruelo GE, Pham SM, Perez EE, Karnik R, Hunter JA, Dauphin DD, Wilkinson JD. Not Altered. CC.
Acute Antibody Mediated Rejection. A) A 4-year-old child who had good allograft function initially and then developed acute antibody-mediated rejection 2 weeks after deceased donor kidney transplantation. Renal biopsy reveals marked acute tubular necrosis and interstitial hemorrhage. There is evidence of glomerulitis and tubulitis (H&E, 40×). B) Immunofluorescence in this patient reveals diffuse C4d staining of the peritubular capillaries, supporting the diagnosis of acute antibody-mediated rejection. Not Altered. CC. Issues in solid-organ transplantation in children: translational research from bench to bedside. Lipshultz SE, Chandar JJ, Rusconi PG, Fornoni A, Abitbol CL, Burke GW, Zilleruelo GE, Pham SM, Perez EE, Karnik R, Hunter JA, Dauphin DD, Wilkinson JD. Not Altered. CC.
Acute Tubular Necrosis (ATN)
Acute tubular necrosis (ATN) is defined as the injury and necrosis of tubular epithelial cells.
Acute tubular necrosis (ATN) is the most common cause of acute renal failure or also called intrarenal azotemia.
Necrotic cells plug and obstruct renal tubules in acute tubular necrosis (ATN).
Obstruction of the renal tubules decreases the glomerular filtration rate (GFR).
The most common feature of acute tubular necrosis (ATN) is having a small amount of urine output which appears to be brown with granular casts.
The tubular epithelium is dysfunctional, which reduces blood urea nitrogen (BUN) reabsorption, serum BUN:Creatinine ratio is less than 15, decreased reabsorption of sodium (FENa > 2%), and inability to concentrate urine (urine osm <500 mOsm/kg).
The etiology of acute tubular necrosis may be classified as either:
- Ischemic
- Nephrotoxic
Ischemic Acute Tubular Necrosis
Ischemic acute tubular necrosis (ATN) happens when tubular cells do not receive enough oxygen.
Ischemic acute tubular necrosis (ATN) is often preceded by prerenal azotemia, an excessively high level of nitrogen waste products in the blood.
The thick ascending limb’s proximal tubule and medullary segment are especially vulnerable to ischemia damage.
Nephrotoxic Acute Tubular Necrosis (ATN)
Nephrotoxic acute tubular necrosis (ATN) occurs when toxic substances are exposed to the tubular cells.
The proximal tubules are extremely susceptible to acute tubular necrosis (ATN).
Causes of nephrotoxic acute tubular necrosis (ATN) includes:
- The most common cause of nephrotoxic acute tubular necrosis (ATN) is aminoglycosides.
- Heavy metals such as lead
- Myoglobinuria for example from crush injury to muscle
- Ethylene glycol which is associated with oxalate crystals in urine
- Radiocontrast dye
- Tumor lysis syndrome (due to urate)
Prior to starting chemotherapy, hydration and allopurinol are used to reduce the risk of tumor lysis syndrome (due to urate) induced acute tubular necrosis (ATN).
Clinical features of acute tubular necrosis (ATN) include:
- Oliguria
- Brown granular casts
- High levels of blood urea nitrogen (BUN) and creatinine
- Metabolic acidosis with hyperkalemia
Although acute tubular necrosis (ATN) illness is treatable because it is considered reversible, supportive dialysis is often needed because electrolyte abnormalities can be lethal.
The symptoms of acute tubular necrosis (ATN), specifically oliguria might last for two to three weeks before the patient’s recovery.
Acute tubular necrosis (ATN) takes time for tubular cells, which are stable cells, to re-enter the cell cycle and regenerate.
Acute Interstitial Nephritis
Acute interstitial nephritis (intrarenal azotemia) is caused by drug-induced hypersensitivity involving the interstitium and tubules.
Etiology of acute interstitial nephritis includes:
- Non-steroidal anti-inflammatory drugs (NSAIDs)
- Penicillin
- Diuretics
Symptoms of acute interstitial nephritis include:
- Oliguria
- Fever
- Rash
The rash associated with acute interstitial nephritis typically will appear days to weeks after starting a drug.
Eosinophils may be found in urine in patients with acute interstitial nephritis.
Symptoms of acute interstitial nephritis may resolve with drug cessation.
Renal papillary necrosis may develop and progress in acute interstitial nephritis.
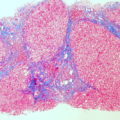
 Acute Interstitial Nephritis. An Unusual Presentation of Classic Idiopathic Polyarteritis Nodosa as Acute Interstitial Nephritis, in Clinical Medicine Insights: Case Reports Libertas Academica. Not altered. CC BY 2.0
Acute Interstitial Nephritis. An Unusual Presentation of Classic Idiopathic Polyarteritis Nodosa as Acute Interstitial Nephritis, in Clinical Medicine Insights: Case Reports Libertas Academica. Not altered. CC BY 2.0


Renal Papillary Necrosis
Renal papillary necrosis is a kidney disorder in which all or some of the renal papillae die.
Renal papillary necrosis is characterized by:
- Gross hematuria
- Flank pain
Risk factors for renal papillary necrosis include:
- Diabetes mellitus
- Sickle cell trait
- Sickle cell disease
- Severe acute pyelonephritis
- Chronic analgesic abuse