Jaundice
Jaundice is yellow discoloration of the skin due to liver injury.
The first indication of jaundice is scleral icterus, which is characterized by yellow discoloration of the sclera.
Jaundice is caused by high blood bilirubin levels, which usually exceed 5.0 mg/dL and rise in response to bilirubin metabolism disruptions.
In order to understand jaundice it is helpful to understand bile production, storage, and secretion:
- Bilirubin is produced when red blood cells (RBCs) are consumed by macrophages of the reticuloendothelial system
- Heme protoporphyrin is transformed to unconjugated bilirubin (UCB)
- This unconjugated bilirubin is transported to the liver via albumin
- Bilirubin is converted into bile by the hepatocyte enzyme uridine glucuronyl transferase (UGT)
- Bile is transmitted to bile canaliculi
- Bile is stored in the gallbladder
- Following a meal the gallbladder releases bile into the duodenum via the ampulla of Vater in order to aid with digestion of lipids and cholesterols
- When intestinal bacteria convert bile to urobilinogen, it causes brown feces
- Bile is also partially filtered by the kidney and reabsorbed into the circulation, turning urine yellow
 Jaundice. A person with jaundice from pancreatic cancer. James Heilman, MD. not altered. CC BY 3.0
Jaundice. A person with jaundice from pancreatic cancer. James Heilman, MD. not altered. CC BY 3.0
Viral Hepatitis
Viral hepatitis is an inflammation of the liver parenchyma due to a viral infection.
Causes of viral hepatitis include:
- Hepatitis virus
- Epstein-Barr virus (EBV)
- Cytomegalovirus (CMV)
Acute hepatitis is caused by the hepatitis virus and can proceed to chronic hepatitis.
Symptoms of viral hepatitis include:
- Jaundice
- Fever
- Malaise
- Nausea
- Increased liver enzymes (ALT > AST)
Hepatocyte apoptosis is a sign of inflammation, which affects the lobules of the liver and the portal tracts.
With high liver enzymes, some of the cases could be asymptomatic.
When symptoms show, they last for usually less than 6 months in acute hepatitis.
Symptoms of chronic hepatitis persist for more than 6 months.
Inflammation mostly affects the portal tract and carries a risk of developing into cirrhosis.
 Viral Hepatitis. High magnification micrograph of ground glass hepatocytes, as seen in a chronic hepatitis B infection with a high viral load. Liver biopsy. H&E stain. Nephron. Not altered. CC BY-SA 3.0
Viral Hepatitis. High magnification micrograph of ground glass hepatocytes, as seen in a chronic hepatitis B infection with a high viral load. Liver biopsy. H&E stain. Nephron. Not altered. CC BY-SA 3.0


Cirrhosis
Cirrhosis is the last stage of liver damage and is marked by bands of fibrosis and hepatocyte regenerating nodules that disrupt the normal hepatic parenchyma.
Under the endothelial cells that line the sinusoids, stellate cells that are present in fibrosis are responsible for cirrhosis.
Clinical features associated with cirrhosis include:
- Jaundice
- Congestive splenomegaly/hypersplenism
- Portosystemic shunts
- Gynecomastia
- Spider angiomas
- Portal hypertension
- Ascites
- Altered mental status (AMS)
- Hepatorenal syndrome
- Impaired detoxification
- Asterixis
- Palmar erythema caused by hyperestrinism
- Hypoalbuminemia
- Edema
- Coagulopathy caused by impaired synthesis of clotting factors
The degree of deficiency is followed by prothrombin time (PT).
 Cirrhosis. Micronodular cirrhosis, with diffuse areas of pallor. Centers for Disease. Dr. Edwin P. Ewing, Jr. Not altered. CC0
Cirrhosis. Micronodular cirrhosis, with diffuse areas of pallor. Centers for Disease. Dr. Edwin P. Ewing, Jr. Not altered. CC0
")










Alcohol Related Liver Disease
Alcohol consumption is the most common reason for liver disease in the West.
Alcohol consumption can cause damage to the hepatic parenchyma, which leads to alcohol related liver disease.
The buildup of fat in hepatocytes causes the liver to become heavy and greasy.
Alcohol consumption can cause chemical damage to hepatocytes alcoholic hepatitis.
A metabolite of alcohol called acetaldehyde induces liver damage.
Hepatocyte swelling and the development of Mallory bodies are it’s defining features.
Cirrhosis is a consequence of long-term, chronic alcohol-induced liver damage that affects 10 – 20% of people who excessively drink alcohol.
 Alcohol Related Liver Disease. microscopy of liver,H&E stain, showing evidence of Alcoholic Hepatitis: fatty change, cell necrosis, Mallory bodies:image from PEIR - University of Alabama at Birmingham Department of Pathology. Not altered. CC BY-SA 2.5.
Alcohol Related Liver Disease. microscopy of liver,H&E stain, showing evidence of Alcoholic Hepatitis: fatty change, cell necrosis, Mallory bodies:image from PEIR - University of Alabama at Birmingham Department of Pathology. Not altered. CC BY-SA 2.5.

Nonalcoholic Fatty Liver Disease (NAFLD)
Nonalcoholic fatty liver disease (NAFLD) is characterized by fatty changes, hepatitis, and/or cirrhosis that occur without the use of alcohol or any other recognized injury, yet it is linked to obesity.
Nonalcoholic fatty liver disease (NAFLD) is a diagnosis of exclusion.
In nonalcoholic fatty liver disease (NAFLD) ALT > AST.
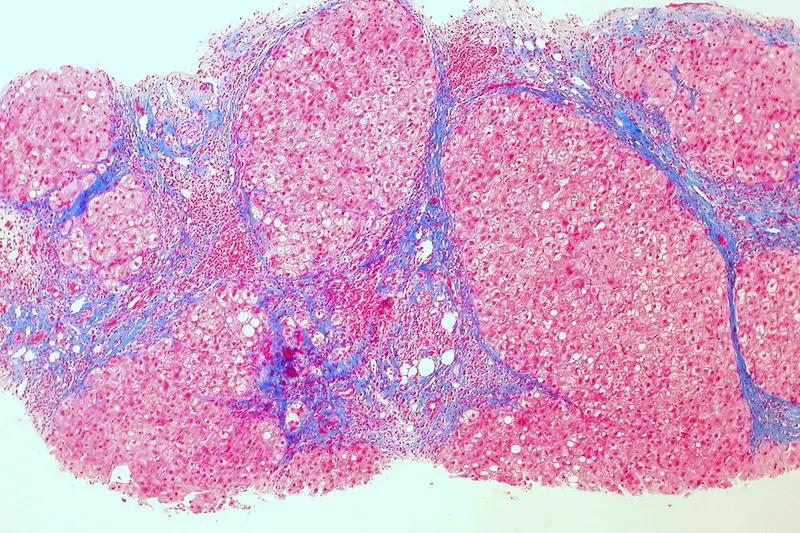
 Nonalcoholic Fatty Liver Disease. Micrograph of non-alcoholic fatty liver disease, demonstrating marked steatosis (fat in liver cells appears white; connective tissue, blue). Trichrome stain Nephron - Not altered. CC BY-SA 3.0
Nonalcoholic Fatty Liver Disease. Micrograph of non-alcoholic fatty liver disease, demonstrating marked steatosis (fat in liver cells appears white; connective tissue, blue). Trichrome stain Nephron - Not altered. CC BY-SA 3.0





Hemochromatosis
Excess bodily iron causes hemosiderosis, which can cause organ damage and tissue deposition in the condition known as hemochromatosis.
Free radical production causes tissue damage, which is mediated by autosomal recessive deficiencies in iron absorption (primary hemochromatosis) or chronic transfusions (secondary hemochromatosis).
The HFE gene, often due to mutation C282Y, is the cause of primary hemochromatosis.
C282Y causes tyrosine takes the place of cysteine at amino acid 282.
Hemochromatosis usually affects adults.
Clinical features of hemochromatosis include:
- Cirrhosis
- Secondary diabetes mellitus
- Bronze skin
- Cardiac arrhythmias
- Gonadal dysfunction
- Testicular atrophy
Lab findings in hemochromatosis include:
- Ferritin (increased)
- Serum iron (increased)
- Percent transferrin saturation (increased)
- Transferrin (decreased)
Liver histology shows that the hepatocytes have accumulated brown pigment.
The brown pigment is lipofuscin, a byproduct of the turnover, wear and tear, and peroxidized lipids.
Prussian blue stain differentiates iron from lipofuscin.
There is an elevated risk of hepatocellular carcinoma in hemochromatosis.
Hemochromatosis is treated by phlebotomy.
 Hemochromatosis. Selective iron deposition (blue) in pancreatic islet beta cells (red) Hotheartdog - Not altered. CC BY-SA 4.0
Hemochromatosis. Selective iron deposition (blue) in pancreatic islet beta cells (red) Hotheartdog - Not altered. CC BY-SA 4.0


Wilson Disease
Wilson disease is due to an ATP7B gene abnormality that affects ATP-mediated hepatocyte copper transport on an autosomal recessive basis.
Wilson disease is characterized by copper not being transported into bile or incorporated into ceruloplasmin.
In Wilson disease, copper accumulates in hepatocytes, leaks into serum, and accumulates in tissues.
Tissue damage results from hydroxyl free radical generation that is mediated by copper.
Wilson disease first appears as:
- Behavioral changes
- Dementia
- Chorea
- Parkinsonian
- Kayser-Fleischer rings on the cornea
Copper buildup in the basal ganglia are examples of neurologic manifestations of Wilson disease.
Laboratory results in Wilson disease show:
- Increased urinary copper (>100 mcg)
- Serum ceruloplasmin
- Copper on liver biopsy
The sole treatment for Wilson disease is D-penicillamine, which chelates copper.
Wilson disease is associated with increased risk for hepatocellular carcinoma.
 Wilson Disease. Kayser-Fleischer ring: copper deposition in Descemet’s membrane of the cornea. These rings can be either dark brown, golden, or reddish-green, are 1 to 3 mm wide, and appear at the corneal limbus. With rare exceptions, they are diagnostic of inherited hepatolenticular degeneration—Wilson’s disease. This 32-year-old patient complained of longstanding difficulty speaking. He also had a tremor. Herbert L. Fred, MD, Hendrik A. van Dijk - Not altered. CC BY 3.0
Wilson Disease. Kayser-Fleischer ring: copper deposition in Descemet’s membrane of the cornea. These rings can be either dark brown, golden, or reddish-green, are 1 to 3 mm wide, and appear at the corneal limbus. With rare exceptions, they are diagnostic of inherited hepatolenticular degeneration—Wilson’s disease. This 32-year-old patient complained of longstanding difficulty speaking. He also had a tremor. Herbert L. Fred, MD, Hendrik A. van Dijk - Not altered. CC BY 3.0




Primary Biliary Cirrhosis
Primary biliary cirrhosis (PBC) is the destruction of intrahepatic bile ducts by autoimmune processes.
Primary biliary cirrhosis (PBC) is associated with granulomatous disease.
Primary biliary cirrhosis (PBC) occurs more often in women who are 40 years of age or older.
Although the etiology of primary biliary cirrhosis (PBC) is unknown, antimitochondrial antibodies are frequently present.
 Primary Biliary Cirrhosis. Intermediate magnification micrograph of primary biliary cirrhosis. Liver biopsy. H&E stain. Features: Bile duct intraepithelial lymphocytes - key feature. Bile duct epithelial cells with eosinophilic cytoplasm. Granulomata - close to the bile duct. Portal inflammation with mixed cell population, i.e. lymphocytes, plasma cells, eosinophils. See also Image:primary biliary cirrhosis low mag.jpg Image:primary biliary cirrhosis intermed mag.jpg Nephron - Not altered. CC BY-SA 3.0
Primary Biliary Cirrhosis. Intermediate magnification micrograph of primary biliary cirrhosis. Liver biopsy. H&E stain. Features: Bile duct intraepithelial lymphocytes - key feature. Bile duct epithelial cells with eosinophilic cytoplasm. Granulomata - close to the bile duct. Portal inflammation with mixed cell population, i.e. lymphocytes, plasma cells, eosinophils. See also Image:primary biliary cirrhosis low mag.jpg Image:primary biliary cirrhosis intermed mag.jpg Nephron - Not altered. CC BY-SA 3.0



Primary Sclerosing Cholangitis
Primary sclerosing cholangitis (PSC) is inflammation and fibrosis of intrahepatic and extrahepatic bile ducts.
Primary sclerosing cholangitis (PSC) has a periductal fibrosis with an onion-skin appearance.
On contrast imaging, uninvolved areas expand, giving them a beaded look.
Primary sclerosing cholangitis has an unknown etiology, but related to ulcerative colitis.
P-ANCA is positive in primary sclerosing cholangitis.
Primary sclerosing cholangitis is associated with:
- Obstructive jaundice
- Cirrhosis
- Cholangiocarcinoma
 Primary Sclerosing Cholangitis. CT scan findings in a case of primary sclerosing cholangitis. Dima Nimri (image) and Akshun Kalia (annotations) - Not altered. CC BY-SA 3.0
Primary Sclerosing Cholangitis. CT scan findings in a case of primary sclerosing cholangitis. Dima Nimri (image) and Akshun Kalia (annotations) - Not altered. CC BY-SA 3.0



Reye Syndrome
Reye syndrome occurs in children with viral illnesses that take aspirin.
Reye syndrome is characterized by:
- Fulminant liver failure
- Encephalopathy
- Hypoglycemia
- Increased liver enzymes
Reye syndrome can result in coma and even death.
 Reye Syndrome. Histopathology of Reye's syndrome, liver Histopathology of autopsy liver from child who died of Reye's syndrome. Hepatocytes are pale-staining due to intracellular fat droplets. CDC/ Dr. Edwin P. Ewing, Jr. Not altered. Public Domain.
Reye Syndrome. Histopathology of Reye's syndrome, liver Histopathology of autopsy liver from child who died of Reye's syndrome. Hepatocytes are pale-staining due to intracellular fat droplets. CDC/ Dr. Edwin P. Ewing, Jr. Not altered. Public Domain.
Hepatic Adenoma
Hepatic adenoma is a benign tumor of the hepatocytes.
Hepatic adenoma development is correlated to the usage of oral contraceptives and goes away when the medication is stopped.
Particularly during pregnancy, there is a danger of rupture and intraperitoneal hemorrhage in patients with hepatic adenoma(s).
These subcapsular tumors spread when exposed to estrogen.
 Hepatic Adenoma. Micrograph of a hepatic adenoma demonstrating a regular reticulin scaffold. Reticulin stain Nephron. Not altered. CC BY-SA 3.0
Hepatic Adenoma. Micrograph of a hepatic adenoma demonstrating a regular reticulin scaffold. Reticulin stain Nephron. Not altered. CC BY-SA 3.0




Hepatocellular Carcinoma (HCC)
Hepatocellular carcinoma (HCC) is the malignant tumor of hepatocytes, in contrast to hepatic adenoma.
Risk factors for hepatocellular carcinoma (HCC) include:
- Chronic hepatitis (HBV and HCV)
- Cirrhosis
- Nonalcoholic fatty liver disease
- Hemochromatosis
- Wilson disease
- A1AT deficiency
- Budd-Chiari syndrome
- Aspergillus infection (due to aflatoxin production)
- Liver infarction
Hepatocellular carcinoma (HCC) presents with severe hepatomegaly and ascites.
The prognosis of hepatocellular carcinoma (HCC) is poor.
Hepatocellular carcinoma (HCC) produces the serum tumor marker alpha-fetoprotein (AFP).
 Hepatocellular Carcinoma. Hepatocellular carcinoma This specimen is from a 50ish woman who presented to the hospital with abdominal pain and ascites. The radiologist recovered what appeared to be whole blood on paracentesis. Cytological exam of the bloody fluid showed no evidence of malignancy. Liver function tests were abnormal, and serologic tests were positive for antibody to hepatitis C. The patient deteriorated rapidly and died within a few days. The autopsy showed this hepatocellular carcinoma occupying much of the volume of a cirrhotic liver. Furthermore, the tumor had invaded the diaphragm and ruptured into the peritoneal cavity, causing the bloody ascites. The photo shows a view of a longitudinal slice taken through the full length of the liver. The photos were shot with a Minolta X-370 with 100 mm bellows lens on Kodak Elite ISO 100 transparency film. The specimen was sliced fresh and fixed in formalin overnight, then briefly immersed in 70% alcohol to retrieve some of the native color and dull the surface reflections. Photograph by Ed Uthman, MD. Public domain. Posted 23 Sep 00 http://web2.airmail.net/uthman/specimens/index.html Permission details. Not altered. Public Domain
Hepatocellular Carcinoma. Hepatocellular carcinoma This specimen is from a 50ish woman who presented to the hospital with abdominal pain and ascites. The radiologist recovered what appeared to be whole blood on paracentesis. Cytological exam of the bloody fluid showed no evidence of malignancy. Liver function tests were abnormal, and serologic tests were positive for antibody to hepatitis C. The patient deteriorated rapidly and died within a few days. The autopsy showed this hepatocellular carcinoma occupying much of the volume of a cirrhotic liver. Furthermore, the tumor had invaded the diaphragm and ruptured into the peritoneal cavity, causing the bloody ascites. The photo shows a view of a longitudinal slice taken through the full length of the liver. The photos were shot with a Minolta X-370 with 100 mm bellows lens on Kodak Elite ISO 100 transparency film. The specimen was sliced fresh and fixed in formalin overnight, then briefly immersed in 70% alcohol to retrieve some of the native color and dull the surface reflections. Photograph by Ed Uthman, MD. Public domain. Posted 23 Sep 00 http://web2.airmail.net/uthman/specimens/index.html Permission details. Not altered. Public Domain


")

")
")
")
")
")


")
")
")

Liver Metastasis
Compared to primary liver tumors, liver metastasis is more common.
Clinical diagnosis of liver metastasis may reveal a nodular free edge of the liver and hepatomegaly.
The most usual sources are liver metastasis are:
- Colon carcinomas
- Pancreatic carcinomas
- Lung cancers
- Breast cancer
Radiology of liver metastasis usually show numerous nodules in the liver.
 Liver Metastasis. Micrograph of a liver core needle biopsy showing metastatic cancer. Nephron - Not altered. CC BY-SA 3.0
Liver Metastasis. Micrograph of a liver core needle biopsy showing metastatic cancer. Nephron - Not altered. CC BY-SA 3.0





