Pulmonary Hypertension Pathology Video
Pulmonary Hypertension
Pulmonary hypertension refers to a form of high blood pressure that affects the pulmonary circuit (mean arterial pressure > 25 mmHg; normal is 10 mmHg).
Pulmonary hypertension condition is characterized by atherosclerosis of the pulmonary trunk, smooth muscle hypertrophy of pulmonary arteries, and intimal fibrosis.
Plexiform lesions are seen with severe, long-standing pulmonary hypertension.
Extreme pulmonary hypertension may lead to right ventricular hypertrophy with eventual cor pulmonale characterized by exertional dyspnea or right-sided heart failure.
Pulmonary hypertension is classified either as primary or secondary based on etiology.
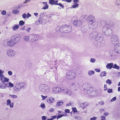
 Pulmonary Hypertension Pathology. Micrograph showing arteries in pulmonary hypertensive with marked thickening of the walls. Yale Rosen. Not altered. CC BY-SA 2.0
Pulmonary Hypertension Pathology. Micrograph showing arteries in pulmonary hypertensive with marked thickening of the walls. Yale Rosen. Not altered. CC BY-SA 2.0

Primary Pulmonary Hypertension
Primary pulmonary hypertension most prevalent among young female adults.
The cause of primary pulmonary hypertension is unknown.
Some familial forms of primary pulmonary hypertension are attributed to the inactivating mutations of BMPR2, causing the proliferation of vascular smooth muscle.
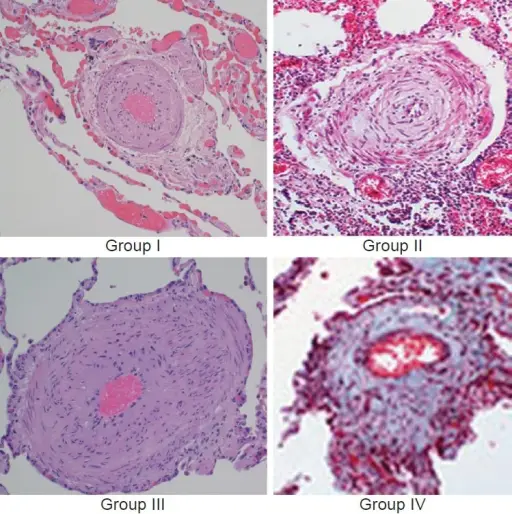
 Obstructive remodelling of a small pulmonary artery in pulmonary arterial hypertension (increased thickness of the three vessel layers and severe lumen reduction are shown) and ongoing pathobiological processes in the different layers of the vessel wall (yellow boxes) and in the blood. Asterisks indicate the potential processes involved. Corrective interactions of the related approved therapeutic interventions are also reported (green boxes). *Vasoconstriction; †Proliferation/migration; ‡Inflammation; §Thrombosis. B-FGF, basic fibroblast growth factor; BMPR, bone morphogenetic protein receptor; [Ca2+], intracellular calcium concentration; K+ch, membrane potassium channels; SMC, smooth muscle cells; MFB, myofibroblasts; MMP, matrix metalloproteases; PDE-5, phosphodiesterase type 5; PDGF, platelet-derived growth factor; TxA2, tromboxane A2; VEGF, vascular endothelial growth factor; VIP, vasoactive intestinal peptide. The pathological picture is a courtesy of Dr Carol Farver, Cleveland Clinic. Pulmonary arterial hypertension: from the kingdom of the near-dead to multiple clinical trial meta-analyses. Galiè N, Palazzini M, Manes A - European heart journal (2010). Not Altered. CC.
Obstructive remodelling of a small pulmonary artery in pulmonary arterial hypertension (increased thickness of the three vessel layers and severe lumen reduction are shown) and ongoing pathobiological processes in the different layers of the vessel wall (yellow boxes) and in the blood. Asterisks indicate the potential processes involved. Corrective interactions of the related approved therapeutic interventions are also reported (green boxes). *Vasoconstriction; †Proliferation/migration; ‡Inflammation; §Thrombosis. B-FGF, basic fibroblast growth factor; BMPR, bone morphogenetic protein receptor; [Ca2+], intracellular calcium concentration; K+ch, membrane potassium channels; SMC, smooth muscle cells; MFB, myofibroblasts; MMP, matrix metalloproteases; PDE-5, phosphodiesterase type 5; PDGF, platelet-derived growth factor; TxA2, tromboxane A2; VEGF, vascular endothelial growth factor; VIP, vasoactive intestinal peptide. The pathological picture is a courtesy of Dr Carol Farver, Cleveland Clinic. Pulmonary arterial hypertension: from the kingdom of the near-dead to multiple clinical trial meta-analyses. Galiè N, Palazzini M, Manes A - European heart journal (2010). Not Altered. CC.
Secondary Pulmonary Hypertension
Secondary pulmonary hypertension is caused by underlying diseases or other known risk factors.
The most common causes are of secondary pulmonary hypertension include:
- Hypoxemia (lung diseases)
- Increased volume in the pulmonary circuit (e.g., congenital heart disease)
Secondary pulmonary hypertension may also arise with recurrent pulmonary embolism.
 Secondary Pulmonary Hypertension. Is a complication of many cardiac, pulmonary, and extrathoracic conditions. Robina Weermeijer. Not altered. CC.
Secondary Pulmonary Hypertension. Is a complication of many cardiac, pulmonary, and extrathoracic conditions. Robina Weermeijer. Not altered. CC.