Subacute cerebellar degeneration is characterized by the deterioration of the area of the brain concerned with muscle coordination and balance.
There are two types of subacute cerebellar degeneration:
- Paraneoplastic cerebellar degeneration due to cancer
- Thiamine deficiency associated cerebellar degeneration, caused by a lack of the vitamin B1 (thiamine) which may be related to alcoholism or a poor diet
What is the Pathology of Subacute Cerebellar Degeneration?
Etiology: The cause of Subacute Cerebellar Degeneration is autoimmune.
Pathogenesis: Autoimmune mediated antibodies and T-cells attacking normal cells in the nervous systems.
How does Subacute Cerebellar Degeneration Present?
Patients with subacute cerebellar degeneration are typically over 50 years of age on average, and females are predominantly affected. The symptoms, features, and clinical findings associated with Subacute Cerebellar Degeneration include ataxia, dysarthria, dysphagia, diplopia, tremors, and vertigo.
How is Subacute Cerebellar Degeneration Diagnosed?
The diagnostic criteria for paraneoplastic subacute cerebellar degeneration are:
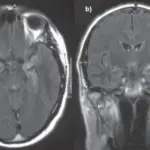
- Severe cerebellar symptoms less than 12 weeks, along with no abnormal sign of cerebellar size reduction
- Rankin scale score of at least a 3, indicating that symptoms interfere with daily life significantly
- Clinical evidence of cerebellar dysfunction, specifically within the trunk or hemispheres, and established diagnosis of cancer within 5 years from the onset of symptoms
- Cerebellar symptoms and cancer-related antibodies
How is Subacute Cerebellar Degeneration Treated?
Subacute cerebellar degeneration is treated by prompt tumor removal, chemotherapy and radiation therapy. Adjuvant therapy with glucocorticoids such as methylprednisolone and immunotherapy with potent T cell inhibition, such as tacrolimus and rituximab may be helpful. Physical therapy and ocupational therapy should aso be considered.
What is the Prognosis of Subacute Cerebellar Degeneration?
The prognosis of subacute cerebellar degeneration is poor. Most symptoms (such as ataxia and vision problems) can be reversed if detected and treated promptly. However, improvement in memory function and cognitive skills may be slow and, usually, incomplete. Without treatment, this condition can be disabling and life-threatening.