Bronchopulmonary dysplasia is a form of chronic lung disease that affects newborns, most often those who are born prematurely and need oxygen therapy.
What is the Pathology of Bronchopulmonary Dysplasia?
The pathology of bronchopulmonary dysplasia is:
–Etiology: The cause of bronchopulmonary dysplasia is damage to the delicate tissue of the lungs. Mostly this disorder develops after a premature baby receives additional oxygen or has been on a ventilator.
–Genes involved: CCL18, NBL1
–Pathogenesis: The sequence of events that lead to bronchopulmonary dysplasia involves various factors which can not only injure small airways but also interfere with alveolar septation. Injury from mechanical ventilation and reactive oxygen species to premature lungs in the presence of antenatal factors predisposing the lungs to bronchopulmonsry dysplasia form the basis of pathogenesis in preterm neonates. An increase in proinflammatory cytokines, tumor necrosis factor alpha and growth factors and angiogenic factors results in aberrant tissue repair and arrest in lung development.
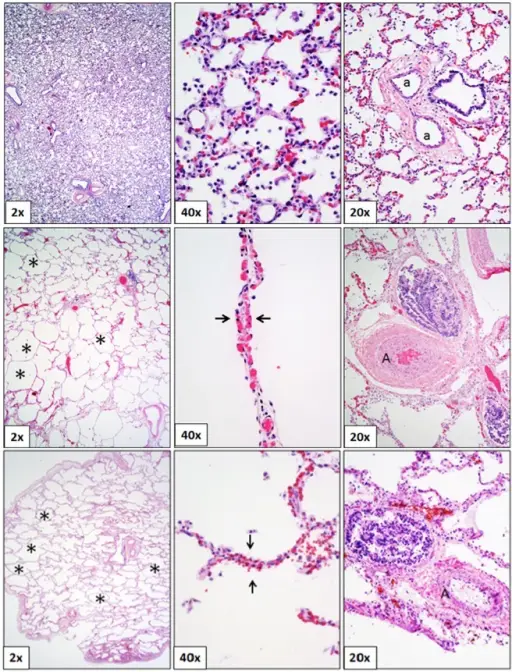
–Morphologic changes: The morphologic changes involved with bronchopulmonary dysplasia are bronchi of the lungs are damaged, causing tissue destruction (dysplasia) in the tiny air sacs of the lung (alveoli).
How does Bronchopulmonary Dysplasia Present?
Patients with bronchopulmonary dysplasia are typically male premature neonates born more than 10 weeks early. The symptoms, features, and clinical findings associated with bronchopulmonary dysplasia include: rapid breathing, wheezing, labored breathing, repeated lung infections and difficulty in feeding.
How is Bronchopulmonary Dysplasia Diagnosed?
Bronchopulmonary dysplasia is diagnosed by chest X-rays, blood tests to check oxygen levels, and echocardiography to check pulmonary hypertension.
How is Bronchopulmonary Dysplasia Treated?
Bronchopulmonary dysplasia has no medical treatment. Treatment focuses good nutrition to help the lungs grow and develop. During this time, babies get breathing and oxygen help so that they can grow and thrive.
What is the Prognosis of Bronchopulmonary Dysplasia?
The prognosis of bronchopulmonary dysplasia is good. Infants with bronchopulmonary dysplasia typically gradually improve after 2 to 4 months of supplemental oxygen or assisted ventilation. Most infants survive, but some infants with very severe disease die even after months of care.

