Dentatorubral-pallidoluysian atrophy is a rare autosomal dominant neurodegenerative disorder clinically characterized by various combinations of cerebellar ataxia, choreoathetosis, myoclonus, epilepsy, dementia, and psychiatric symptoms.
What is the Pathology of Dentatorubral-Pallidoluysian Atrophy?
The pathology of Dentatorubral-pallidoluysian atrophy is:
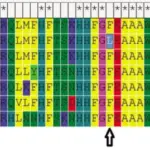
-Etiology: The cause of dentatorubral-pallidoluysian atrophy is unstable expansion of CAG repeats coding for polyglutamine stretches located in exon 5 of the DRPLA gene.
-Genes involved: Atrophin-1 gene.
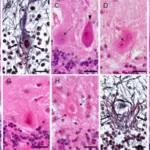
-Pathogenesis: The sequence of events that lead to dentatorubral-pallidoluysian atrophy are due to unstable expansion of CAG repeats coding for polyglutamine stretches located in exon 5 of the DRPLA gene. Dentatorubral-pallidoluysian is characterized by marked, generalized brain atrophy and the accumulation of atrophin-1 with expanded glutamine stretches. Mutant atrophin-1 proteins have been found in neuronal intranuclear inclusions (NII) and diffusely accumulated in the neuronal nuclei. While the role of NIIs (pathologic or protective) is unclear, the diffuse accumulation of mutant protein is regarded as toxic.
How does Dentatorubral-Pallidoluysian Atrophy Present?
Patients with dentatorubral-pallidoluysian typically affects either male or female present at varying age ranges. The symptoms, features, and clinical findings associated with dentatorubral-pallidoluysian atrophy include myoclonus, seizures of different types, behavioral changes, progressive intellectual disability and deterioration, and ataxia. When it begins after the age of 20 years it presents with: ataxia, choreoathetosis or dystonia, delusions, and dementia.
How is Dentatorubral-Pallidoluysian Atrophy Diagnosed?
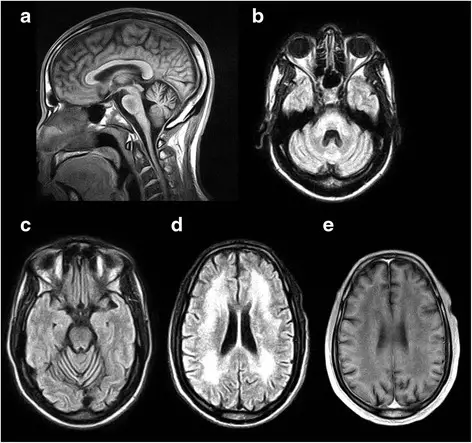
Dentatorubral-pallidoluysian atrophy is diagnosed based on positive family history, clinical findings, and genetic testing. To quantify the extent of the disease, an MRI, EEG and neuropsychological testing are recommended.
How is Dentatorubral-Pallidoluysian Atrophy Treated?
Dentatorubral-pallidoluysian atrophy is treated with anticonvulsants if seizures are present. Psychotropic medications may help with psychiatric disturbances. Physical therapy has also been recommended to maintain function as the condition progresses and occupational therapy to focus on activities of daily living, advice for carers and adaptation to the environment.
What is the Prognosis of Dentatorubral-Pallidoluysian Atrophy?
The prognosis of Dentatorubral-pallidoluysian atrophy is poor. Seizures and dysphagia with frequent fluid and food aspiration cause bronchopneumonia and subsequent death.