Chronic Obstructive Pulmonary Disease Pathology Video
Chronic Obstructive Pulmonary Disease (COPD)
Airflow obstruction from the lungs is a symptom of chronic obstructive pulmonary disease (COPD).
Chronic obstructive pulmonary disease (COPD) is a chronic inflammatory lung disease.
A triad of disorders are associated with chronic obstructive pulmonary disease (COPD), which include:
- Asthma
- Emphysema
- Chronic bronchitis
Chronic obstructive pulmonary disease (COPD) is characterized by airway obstruction.
In chronic obstructive pulmonary disease (COPD), the lung is not empty, and air is trapped.
In chronic obstructive pulmonary disease (COPD), the volume of air that can be forcefully expired is decreased (FVC), especially during the first second of expiration (FEV1); results in an increased FEV1:FVC ratio
Total lung capacity (TLC) refers to the amount of air in the lungs during maximum inflation.
Total lung capacity (TLC) is usually increased due to air trapping.
Due to air trapping, total lung capacity (TLC) often rises in chronic obstructive pulmonary disease.
 Chronic Obstructive Pulmonary Disease. Signs and symptoms of stages of COPD. Mikael Häggström - Not altered. Public Domain
Chronic Obstructive Pulmonary Disease. Signs and symptoms of stages of COPD. Mikael Häggström - Not altered. Public Domain


Chronic Bronchitis
A long-term inflammation of the bronchi is known as chronic bronchitis.
This productive cough of chronic bronchitis persists for at least 3 months throughout a minimum of 2 years.
Chronic bronchitis is strongly linked to smoking.
The enlargement of bronchial mucin glands is a hallmark finding of chronic bronchitis.
Chronic bronchitis causes the mucus glands to be thicker in comparison to the total thickness of the bronchial wall.
In chronic bronchitis the Reid index increases to greater than 50% when the normal Reid index is less than 40%.
Clinical features of chronic bronchitis include:
- Cough
- Cyanosis
A productive cough caused by increased mucus production is a clinical symptom of chronic obstructive pulmonary disease.
Another sign is cyanosis, which is brought on by hypoxia and the carbon dioxide that is trapped by mucus plugs in the skin. This phenomenon is described as “blue bloaters.”
Increased PaCO2 and increased risk of infection are common in this condition.
Another aspect of this condition is called cor pulmonale, which results in the failure of the right side of the heart.
 Morphology and immunohistochemistry of COPD-associated lung lesions. A: Chronic bronchitis. B: Centriacinar emphysema. C: Advanced active bronchitis with fibrosis and emphysema. A-C, hematoxylin-eosin staining; D: CD68-PPARG coexpression with double IHC staining using alkaline phosphatase [red cytoplasm-CD68] and diamino-benzidine [brown nuclei-PPARG]. E: Cells with red fluorescence and green nuclei DCSign-PPARG double fluorescence staining. Nuclear counter-staining is DAPI. Indications: b, bronchus; a, alveolar spaces; arrows, alveolar macrophages. Original magnifications: A-D 20×; E 40×. Analyses of association between PPAR gamma and EPHX1 polymorphisms and susceptibility to COPD in a Hungarian cohort, a case-control study. Penyige A, Poliska S, Csanky E, Scholtz B, Dezso B, Schmelczer I, Kilty I, Takacs L, Nagy L - BMC medical genetics (2010). Not Altered. CC.
Morphology and immunohistochemistry of COPD-associated lung lesions. A: Chronic bronchitis. B: Centriacinar emphysema. C: Advanced active bronchitis with fibrosis and emphysema. A-C, hematoxylin-eosin staining; D: CD68-PPARG coexpression with double IHC staining using alkaline phosphatase [red cytoplasm-CD68] and diamino-benzidine [brown nuclei-PPARG]. E: Cells with red fluorescence and green nuclei DCSign-PPARG double fluorescence staining. Nuclear counter-staining is DAPI. Indications: b, bronchus; a, alveolar spaces; arrows, alveolar macrophages. Original magnifications: A-D 20×; E 40×. Analyses of association between PPAR gamma and EPHX1 polymorphisms and susceptibility to COPD in a Hungarian cohort, a case-control study. Penyige A, Poliska S, Csanky E, Scholtz B, Dezso B, Schmelczer I, Kilty I, Takacs L, Nagy L - BMC medical genetics (2010). Not Altered. CC.


Emphysema
The structural alteration of the lung parenchyma characterizes emphysema.
Alveolar air sacs are destroyed in emphysema.
In emphysema, during exhalation, the airways contract and lose their elastic recoil, causing blockage and air entrapment.
The pathogenesis of emphysema involves:
- Neutrophils and macrophages typically release proteases in response to lung inflammation because of an imbalance of proteases and antiproteases
- Alpha-1-antitrypsin (A1AT) attempts to neutralize proteases
- Excessive inflammation or lack of A1AT leads to destruction of the alveolar air sacs
Emphysema most commonly results from smoking.
Pollutants in smoke lead to excessive inflammation and protease-mediated damage.
Smoking induced emphysema is typically centriacinar, which manifests most severely in the upper lobes.
A1AT deficiency is a rare cause of emphysema, which is usually panacinar that is most severe in the lower lobes.
Liver cirrhosis may also be present in A1AT definiency due to abnormal enzyme production in the liver.
- The misfolding of the mutant protein is what causes A1AT deficiency
- Damage to the liver occurs as a result of the accumulation of mutant A1AT in the hepatocyte endoplasmic reticulum
Histopathology of a liver biopsy from a patient with A1AT deficiency shows pink, periodic acid Schiff (PAS) positive globules in hepatocytes.
The degree of AlAT deficiency determines how severe the disease is.
PiMMnormal > PiZM > PiZZworse.
PiM is the normal allele.
Two copies are usually expressed (PiMM).
PiZ is the most common clinically relevant mutation.
PiZ results in significantly low levels of circulating AIAT.
Although PiMZ heterozygotes often have lower levels of AlAT in their blood, there is a high risk of developing emphysema if they smoke.
PiZZ homozygotes are at a higher risk of developing cirrhosis and panacinar emphysema.
Clinical symptoms of emphysema include:
- Dyspnea
- Dry cough
- Protracted expiration with pursed lips, or “pink-puffer”
- Weight loss
- Hypoxemia due to damaged capillaries in the alveolar sac
- Cor pulmonale
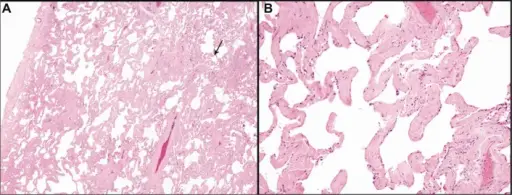
 Restrictive Lung Diseases Pathology. Low magnification micrograph of emphysema. H&E stain. The left of image shows severe emphysema (large empty spaces). The lung tissue on the right of the image has relative preservation of the alveoli. The top of the image is very near the pleural surface. Nephron. Not altered. CC BY-SA 3.0
Restrictive Lung Diseases Pathology. Low magnification micrograph of emphysema. H&E stain. The left of image shows severe emphysema (large empty spaces). The lung tissue on the right of the image has relative preservation of the alveoli. The top of the image is very near the pleural surface. Nephron. Not altered. CC BY-SA 3.0




Asthma
A reversible bronchoconstriction of the airways brought on most frequently by allergic stimuli, type I hypersensitivity, called asthma.
Childhood is when this condition first manifests.
Eczema, allergic rhinitis, and a history of atopy in the family are frequently linked to it.
The TH2 phenotype is induced by allergens in CD4+T cells of genetically sensitive people.
IgE class switching is mediated by IL-4 secreted by TH2 cells.
On the other hand, IL-5 attracts eosinophils, IL-10 promotes TH2 cells, and TH1 is inhibited by IL-10.
The activation of mast cells by IgE is triggered by reexposure to the allergen.
Bronchoconstriction, inflammation, and edema are the results of leukotrienes C4, D4, and E4 production and release, which is an early phase reaction.
A late-phase reaction results from inflammation, particularly when it produces major basic protein from eosinophils, which damages cells and causes bronchoconstriction to persist.
Clinical features are episodic and related to allergen exposure, and include:
- Dyspnea
- Wheezing
- Cough
The cough is classically with spiral-shaped mucus plugs called Curschmann spirals and eosinophil-derived crystals or Charcot-Leyden crystals.
Status asthmaticus and mortality can be the results of severe, persistent attacks.
In addition to allergy triggers, non-allergic factors that might cause asthma include:
- Exercise
- Viral infections
- Occupational exposures
- Aspirin consumption
 Asthma Curshman’s Spiral. Curschmann's spirals. From one of the pathogists at work. Not altered. CC.
Asthma Curshman’s Spiral. Curschmann's spirals. From one of the pathogists at work. Not altered. CC.




Bronchiectasis
This is the condition where there is a permanent dilation of bronchioles and bronchi and loss of airway tone results in air trapping.
Bronchiectasis is associated with:
- Cystic fibrosis
- Kartagener syndrome
- Tumor
- Foreign body
- Necrotizing infections
- Aspergillus
Cystic fibrosis and Kartagener syndrome are two causes that result in necrotizing inflammation and destruction to the airway walls.
Cystic fibrosis is due to abnormal chloride channels.
Kartagener syndrome is due to dynein arm deficiency that is inherited and prevents the cilia from moving.
Kartagener syndrome is associated with:
- Situs inversus (e.g. heart is on the right side of thorax)
- Sinusitis
- Infertility (due to poor motility of sperm due to aberrent microtubules in the tail)
Aspergillus hypersensitivity causes allergic bronchopulmonary aspergillosis, which results in chronic inflammatory damage.
Individuals with cystic fibrosis or asthma commonly experience allergic bronchopulmonary aspergillosis (ABA).
Complications include hypoxia with cor pulmonale and secondary (AA) amyloidosis are experience.
 Bronchiectasis. CT scan of the lungs showing findings diagnostic of bronchiectasis. White and black arrows point to dilated bronchi characteristic of the disease. Mcgfowler. Not altered. CC BY-SA 3.0
Bronchiectasis. CT scan of the lungs showing findings diagnostic of bronchiectasis. White and black arrows point to dilated bronchi characteristic of the disease. Mcgfowler. Not altered. CC BY-SA 3.0






