Joint pathology is the study of diseases and disorders that effect the joints.
In this section we will focus on the following joint pathology:
- Osteoarthritis
- Rheumatoid arthritis
- Seronegative spondyloarthropathies (ankylosing spondylitis, Reiter syndrome, psoriatic arthritis)
- Infectious arthritis
- Gout
- Pseudogout
Joint
The link between two bones is made by joints.
In general, there are three (3) types of joints:
- Fibrous
- Cartilaginous
- Synovial
Cranial sutures are solid fibrous joints that are securely attached to provide structural support.
Synovial joints have a joint gap that permits motion.
For synovial joints, a joint capsule surrounds the hyaline cartilage that makes up the articular surface of adjacent bones.
In order to lubricate synovial joints and promote fluid mobility, the synovium lining of the joint capsule secretes fluid that is high in hyaluronic acid.
 Joint. - Not altered. CC BY-SA 3.0
Joint. - Not altered. CC BY-SA 3.0


Degenerative Joint Disease
Osteoarthritis
Osteoarthritis is due to wear and tear that results in articular cartilage degeneration over time in degenerative joint disease.
This type of arthritis is the most prevalent in the elderly.
Risk factors for osteoarthritis include:
- Being 60-years-old or older
- Obesity
Osteoarthritis is known as oligoarticular because it only affects a few joints.
Common sites of osteoarthritis include:
- Knees
- Lower lumbar spine
- Hips
- Finger joints (proximal (PIP) and distal (DIP) interphalangeal joints)
Common symptoms of osteoarthritis include:
- Joint stiffness in the morning
- Joint stiffness that becomes worse throughout the day
- Joint stiffness that worsens with activity
Pathologic assessment will show absent of disrupted cartilage on the articular surface of the joint.
Eburnation (eroded cartilage) and osteophytes (bony outgrowths) are classically seen in osteoarthritis.
Fragments of cartilage floating in the joint space are called joint mice.
Additionally, osteophyte formation that typically develops in the distal interphalangeal (DIP) (Heberden nodes) and proximal interphalangeal (PIP) (Bouchard nodes) joints of the fingers.
 Osteoarthritis. Damaged cartilage from sows. (a) cartilage erosion (b)cartilage ulceration (c)cartilage repair (d)osteophyte (bone spur) formation. Rikke K Kirk, Bente Jørgensen, Henrik E Jensen - Not altered. CC BY 2.0
Osteoarthritis. Damaged cartilage from sows. (a) cartilage erosion (b)cartilage ulceration (c)cartilage repair (d)osteophyte (bone spur) formation. Rikke K Kirk, Bente Jørgensen, Henrik E Jensen - Not altered. CC BY 2.0









Rheumatoid Arthritis (RA)
Rheumatoid arthritis (RA) is a chronic, systemic autoimmune condition.
Rheumatoid arthritis (RA) typically affects women above childbearing age.
Rheumatoid arthritis (RA) is linked to HLA-DR4 and is distinguished by joint involvement.
The hallmarks of rheumatoid arthritis (RA) include:
- Synovitis
- Pannus formation
- Inflammatory granulation tissue
Rheumatoid arthritis (RA) may result in joint ankylosis (fusion) and cartilage degradation.
There are several clinical features that can be seen in rheumatoid arthritis (RA) which include:
- Morning stiffness that gets better with movement
- Symmetric involvement of the proximal interphalangeal (PIP) joints in the fingers
- Swan-neck deformity
- Wrist or ulnar deviation
- Pain in the knees, ankles, and elbows
- Distal interphalangeal (DIP) joints are usually spared (unlike osteoarthritis)
- Fevers
- Weight loss
- Malaise
- Myalgia
- Baker cyst or enlargement of the bursa below the knee
- Pleural effusions
- Lymphadenopathy
- Interstitial lung fibrosis
Radiology of rheumatoid arthritis (RA) classically shows osteopenia, cartilage loss, and a narrowing of the joint space on X-ray.
The Fc component of IgG, a rheumatoid factor, is the target of an IgM autoantibody.
Synovial fluid tests of rheumatoid arthritis (RA) show:
- Increased neutrophils
- Increased protein
- Decreased glucose
Complications of rheumatoid arthritis (RA) include:
- Anemia of chronic disease
- Secondary amyloidosis
 Rheumatoid Arthritis. X-ray of the hand in rheumatoid arthritis. Bernd Brägelmann Braegel. Not altered. CC BY 3.0
Rheumatoid Arthritis. X-ray of the hand in rheumatoid arthritis. Bernd Brägelmann Braegel. Not altered. CC BY 3.0





Seronegative Spondyloarthropathies
Lack of rheumatoid factor is one of the characteristics of this group of joint disorders.
HLA-B27 involvement and the axial skeleton are associated.
The sacroiliac joints and spine are affected by ankylosing spondyloarthritis, which develops in young adults, most frequently in men.
Low back pain is one of the symptoms of seronegative spondyloarthropathies.
Eventually, the involvement of vertebral bodies appears, causing the vertebrae to fuse together or form a bamboo spine.
Extra-articular manifestations of ankylosing spondyloarthritis include:
- Uveitis
- Aortitis leading to aortic regurgitation
- Reiter syndrome
Reiter syndrome also includes the triad of:
- Conjunctivitis
- Urethritis
- Arthritis
Reiter syndrome appears in young individuals, mainly men, weeks after an infection with Chlamydia trachomatis.
Psoriatic arthritis is seen in 10% cases of patients with psoriasis.
Psoriatic arthritis typically involves axial and peripheral joints, and the most common afflicted DIP joints are those in the hands and feet, which can result in sausage fingers or toes.
Psoriatic arthritis is associated with scaly rashes.
 Seronegative Spondyloarthropathies. Bone scintigraphy made with 99mTc demonstrating the highly enhanced tumor borders and the left elbow affected by psoriatic arthritis. Panagiotis V Kitsoulis, Georgios Paraskevas, Aristidis Vrettakos and Aikaterini Marini; Not altered. CC BY-SA 2.0
Seronegative Spondyloarthropathies. Bone scintigraphy made with 99mTc demonstrating the highly enhanced tumor borders and the left elbow affected by psoriatic arthritis. Panagiotis V Kitsoulis, Georgios Paraskevas, Aristidis Vrettakos and Aikaterini Marini; Not altered. CC BY-SA 2.0

Infectious Arthritis
A bacterial infection of the joint space that causes inflammation is infectious arthritis.
Neisseria gonorrhoeae in young adults, which is the most frequent cause, is one example of a bacterial cause of infectious arthritis.
Staphylococcus aureus, the second most prevalent cause of infectious arthritis, is a factor that affects older kids and adults.
The knee is the typical affected joint of infectious arthritis, and it typically manifests as a heated joint with restricted range of motion.
Infectious arthritis causes an elevated erythrocyte sedimentation rate (ESR), leukocytosis (a raised white blood cell count), and fever.
 Magnification :40 × Stain :haematoxylin and eosin. A Case of Septic Arthritis of Shoulder Presenting as Stiffness of the Shoulder: Journal of Orthopaedic Case Reports. Not altered. CC.
Magnification :40 × Stain :haematoxylin and eosin. A Case of Septic Arthritis of Shoulder Presenting as Stiffness of the Shoulder: Journal of Orthopaedic Case Reports. Not altered. CC.



Gout
Gout is due to monosodium urate (MSU) crystal deposition in tissues, particularly the joints, as a result of hyperuricemia.
Gout is connected to uric acid overproduction or decreased uric acid excretion.
Purine metabolism produces uric acid, which the kidney excretes.
The most prevalent kind of gout is primary, however the cause of hyperuricemia is uncertain.
Monosodium urate (MSU) crystals deposit in the joint, triggering an acute inflammatory reaction.
Secondary gout is observed in patients with leukemia and myeloproliferative diseases due to increased cell turnover that causes hyperuricemia.
Lesch-Nyhan syndrome which is a X-linked deficiency of hypoxanthine-guanine phosphoribosyltransferase (HGPRT) presents with mental retardation, self-mutilation, and gout.
Reduced renal excretion of uric acid is a sign of renal insufficiency.
Podagra, an excruciatingly painful great toe arthritis, is the classic manifestation of gout.
Risk factors for gout include:
- Alcohol consumption
- Cured meat consumption (salami, pepperoni, etc.)
Gout classically has tophi, which are white, chalky, and form along with fibrosis and a giant cell response.
In the soft tissue and joints of people with chronic gout, uric acid crystal can accumulate into aggregates called gouty tophi.
Laboratory results of gout typically show hyperuricemia.
Urate crystals associated with gout can accumulate in the kidney tubules, and may result in renal failure (urate nephropathy).
Histology of gout shows yellow needle-shaped crystals with negative birefringence under polarized light.
Gout treatments include:
- Lifestyle modification
- Nonsteroidal anti-inflammatory drugs (NSAIDs)
- Colchicine
- Allopurinol
 Gout. Gout presenting as slight redness in the metatarsal–phalangeal joint of the big toe James Heilman, MD - Not altered. CC BY-SA 3.0
Gout. Gout presenting as slight redness in the metatarsal–phalangeal joint of the big toe James Heilman, MD - Not altered. CC BY-SA 3.0








Pseudogout
Pseudogout results from calcium pyrophosphate dihydrate (CPPD) deposition.
Clinically, pseudo-gout is similar to gout.
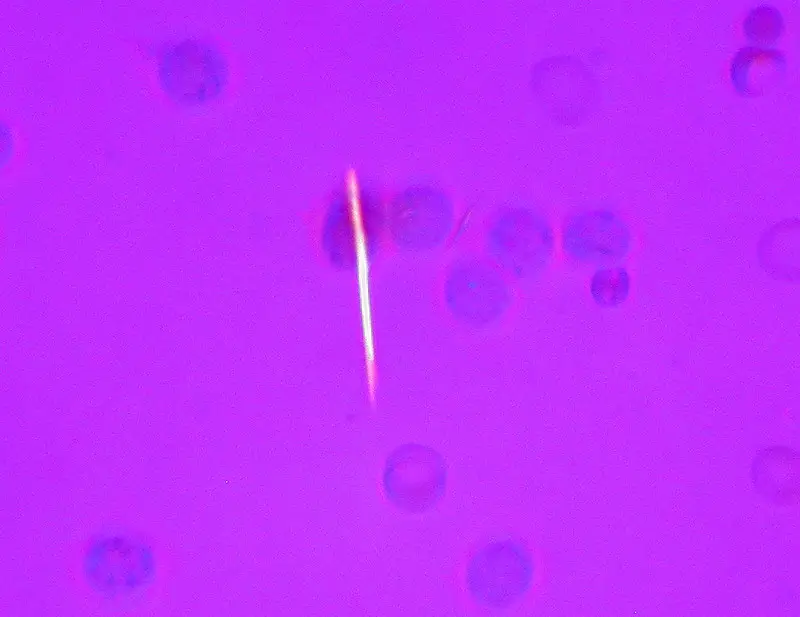
In pseudogout, synovial fluid exhibits rhomboid-shaped crystals with weakly positive birefringence under polarized light.
 Pseudogout. Microscopy with polarized light of tissue by a metatarsal joint, showing crystals whereof some (one annotated) have rhomboid shape and weak positive nirefringence, consistent with calcium pyrophosphate dihydrate crystal deposition disease (pseudogout). Mikael Häggström, M.D Not altered. CC0
Pseudogout. Microscopy with polarized light of tissue by a metatarsal joint, showing crystals whereof some (one annotated) have rhomboid shape and weak positive nirefringence, consistent with calcium pyrophosphate dihydrate crystal deposition disease (pseudogout). Mikael Häggström, M.D Not altered. CC0