Leukopenia and Leukocytosis
Leukopenia and Leukocytosis Pathology Video
Hematopoiesis is a stepwise maturation of CD34+ hematopoietic stem cells.
From the bone marrow, hematopoietic cells develop and are released into the blood.
A white blood cell (WBC) count of 5,000 – 10,000 WBCs per microliter is considered normal.
Leukopenia is a low white blood cell (WBC) count, below 5,000 WBCs per microliter.
Leukocytosis is a high white blood cell (WBC) count, greater than 10,000 WBCs per microliter.
A decrease in one particular cell lineage or an increase in another is typically the cause of a low or high white blood cell (WBC) count.
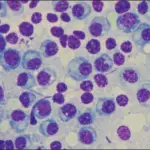
 Leukopenia and Leukocytosis Pathology. Infectious mononucleosis, peripheral smear, high power showing reactive lymphocytes. Ed Uthman, MD. Not altered. CC BY 2.0
Leukopenia and Leukocytosis Pathology. Infectious mononucleosis, peripheral smear, high power showing reactive lymphocytes. Ed Uthman, MD. Not altered. CC BY 2.0
Leukopenia
Leukopenia is a low WBC count, below 5,000 WBCs per microliter.
Neutropenia is a reduction in the amount of circulating neutrophils.
Causes of neutropenia include:
- Drug toxicity, such as stem cell damage from chemotherapy with alkylating drugs, reduces the generation of WBCs, particularly neutrophils
- A severe infection (such as gram-negative sepsis) causes more neutrophils to enter the tissues, which lowers the amount of circulating neutrophils
- Pharmacologically, GM-CSF or G-CSF can be administered to increase granulocyte production and lower infection risk
Lymphopenia is a decreased amount of lymphocytes.
Causes of lymphopenia include:
- Immunodeficiency
- High cortisol state
- Autoimmune destruction
- Radiation therapy
 (a) Peripheral blood (Wright-Giemsa, 100x) showed leukopenia with neutropenia and circulating pseudo-Pelger-Huet cells with bilobed hyposegmented nuclei. Peripheral blood also showed mild normocytic anemia and thrombocytopenia. (b) Bone marrow aspirate (Wright-Giemsa, 100x) showing a mild increase in blasts (7% of cellularity) with a high nuclear to cytoplasmic ratio, vesicular chromatin, and prominent nucleoli with variable granularity. Translocation (6;15)(q12;q15): A Novel Mutation in a Patient with Therapy-Related Myelodysplastic Syndrome: Ali SF, Sonu RJ, Dwyre DM, Jonas BA, Rashidi HH - Case reports in hematology (2015). Not altered. CC.
(a) Peripheral blood (Wright-Giemsa, 100x) showed leukopenia with neutropenia and circulating pseudo-Pelger-Huet cells with bilobed hyposegmented nuclei. Peripheral blood also showed mild normocytic anemia and thrombocytopenia. (b) Bone marrow aspirate (Wright-Giemsa, 100x) showing a mild increase in blasts (7% of cellularity) with a high nuclear to cytoplasmic ratio, vesicular chromatin, and prominent nucleoli with variable granularity. Translocation (6;15)(q12;q15): A Novel Mutation in a Patient with Therapy-Related Myelodysplastic Syndrome: Ali SF, Sonu RJ, Dwyre DM, Jonas BA, Rashidi HH - Case reports in hematology (2015). Not altered. CC.
Leukocytosis
Leukocytosis is a high white blood cell (WBC) count, greater than 10,000 WBCs per microliter.
Increased levels of neutrophils in the blood are known as neutrophilic leukocytosis.
Causes of neutrophilic leukocytosis include:
- Bacterial infection
- Tissue necrosis
Reduced Fc receptors (CD16) characterize immature cells
High levels of cortisol inhibit leukocyte adhesion, which causes a marginated pool of neutrophils to be released
Increased circulating monocytes are referred to as monocytosis.
Causes of monocytosis include:
- Malignancy
- Chronic inflammatory conditions (such as autoimmune and infectious diseases)
Increased circulating eosinophils are referred to as eosinophilia.
Causes of eosinophila include:
- Allergic reactions (type I hypersensitivity reactions)
- Parasitic infections
- Helminth infections
- Hodgkin lymphoma
Eosinophilia is usually associated with IL-5.
Basophilia is the term for elevated basophil counts in the blood.
Basophilia is a condition that is characterized by increased basophils.
Basophilia is a common feature of chronic myeloid leukemia (CML).
Increased circulating lymphocytes are referred to as lymphocytic leukocytosis.
Causes of lymphocytic leukocytosis include:
- Viral infections
- Bordetella pertussis (via lymphocytosis promoting factor)
 (A) Heavy, perivascular and interstitial neutrophilic infiltration (arrowhead) are present (H&E stain, ×40). (B) Fibrinoid necrosis of the small blood vessels with fibrin extravasation and leukocytosis forming nuclear dust (arrowhead) are visible on skin biopsy (H&E stain, ×200). Pulmonary Leukocytoclastic Vasculitis as an Initial Presentation of Myelodysplastic Syndrome: Tuberculosis and Respiratory Diseases. Not altered. CC.
(A) Heavy, perivascular and interstitial neutrophilic infiltration (arrowhead) are present (H&E stain, ×40). (B) Fibrinoid necrosis of the small blood vessels with fibrin extravasation and leukocytosis forming nuclear dust (arrowhead) are visible on skin biopsy (H&E stain, ×200). Pulmonary Leukocytoclastic Vasculitis as an Initial Presentation of Myelodysplastic Syndrome: Tuberculosis and Respiratory Diseases. Not altered. CC.

Infectious Mononucleosis (IM)
Infectious mononucleosis causes reactive CD8+ T cells to increase and present as lymphocytic leukocytosis.
Infectious mononucleosis (IM) is caused viral infections:
- Epstein Barr virus (EBV) (most commonly)
- Cytomegalovirus (CMV) (occasionally)
Epstein Barr virus (EBV) is a saliva-borne infection that typically affects teenagers (“kissing illness”).
Epstein Barr virus (EBV) primarily causes pharyngitis by infecting the oropharynx.
Symptoms of infectious mononucleosis (IM) include:
- Lymphadenopathy
- Splenomegaly
- Hepatomegaly
Due to T-cell hyperplasia in the lymph node paracortex from the CD8+ T-cell response the patient experiences widespread lymphadenopathy.
T-cell hyperplasia in the periarterial lymphatic sheath is the cause of splenomegaly.
Hepatitis with hepatomegaly and increased liver enzyme levels is caused by the liver injury and infiltration.
Laboratory findings of infectious mononucleosis (IM) include:
- High white blood cell (WBC) count
- Leukocytosis
- Atypical lymphocytes (reactive CD8+ T cells) on peripheral blood smear
- Positive monospot test
- IgM antibodies that react with horse or sheep red blood cells are detected (heterophile antibodies)
- The Epstein Barr virus (EBV) viral capsid antigen is detected using serologic testing to provide a definitive diagnosis
Note that it may take about a week of infection for the antibodies to be detected in infectious mononucleosis (IM).
Infectious mononucleosis (IM) may have cytomegalovirus (CMV) as a probable etiology if the monospot test results are negative.
Complications of infectious mononucleosis (IM) include:
- Higher risk for splenic rupture
- Recurrence of infectious mononucleosis
- B-cell lymphoma
The virus’s dormancy in B cells increases the likelihood of recurrence and B-cell lymphoma.
Patients are advised to refrain from contact sports for a year.
Patients can literally rapidly die due to hemorrhage from a splenic rupture associated with of infectious mononucleosis (IM).
It cannot be overstressed to advise against contact sports and activities!
 Infectious Mononucleosis. Lyphadenopathy in someone with mononucleosis James Heilman, MD - Not altered. CC BY-SA 3.0
Infectious Mononucleosis. Lyphadenopathy in someone with mononucleosis James Heilman, MD - Not altered. CC BY-SA 3.0