Nephrotic Syndrome Pathology Video
Nephrotic Syndrome
Nephrotic syndrome is characterized by proteinuria and glomerular disorders leading to hypoalbuminemia-pitting edema.
Nephrotic syndromes include:
- Minimal change disease
- Focal segmental glomerulosclerosis (FSGS)
- Membranous nephropathy
- Membranoproliferative glomerulonephritis (MPGN)
- Diabetes mellitus
- Systemic amyloidosis
Complications of nephrotic syndrome includes:
- Hypogammaglobulinemia increases the risk of infection
- Hypercoagulable state because of loss of antithrombin I (fibrin)
- Hyperlipidemia
- Hypercholesterolemia
 Nephrotic Syndrome. Urinalysis will be able to detect high levels of proteins and occasionally microscopic haematuria. - Not altered. CC BY 2.5
Nephrotic Syndrome. Urinalysis will be able to detect high levels of proteins and occasionally microscopic haematuria. - Not altered. CC BY 2.5







Minimal Change Disease
Minimal change disease is the most prevalent cause of nephrotic syndrome in children.
Minimal change disease is typically idiopathic.
Minimal change disease can be linked to Hodgkin lymphoma.
The kidney histology looks normal in minimal change disease (“minimal change” disease).
Electron microscopy is needed to see the pathology of minimal change disease.
Electron microscopy of minimal change disease shows podocyte foot effacement.
Selective proteinuria may be present because loss of albumin, but not immunoglobulin.
Minimal change disease is treated with steroids.
 Minimal Change Disease. A schematic of the changes seen under the electron microscope of minimal change disease. M Komorniczak. Not altered. CC BY-SA 3.0
Minimal Change Disease. A schematic of the changes seen under the electron microscope of minimal change disease. M Komorniczak. Not altered. CC BY-SA 3.0


Focal Segmental Glomerulosclerosis (FSGS)
Focal segmental glomerulosclerosis (FSGS) is the most common cause of nephrotic syndrome.
Ethnicities at risk of focal segmental glomerulosclerosis (FSGS) include:
- Hispanics
- Americans of African descent
Focal segmental glomerulosclerosis (FSGS) can be linked to HIV infection, heroin use, and sickle cell disease.
Histology of focal segmental glomerulosclerosis (FSGS) shows segmental (some glomeruli) and focal (part of effected glomeruli) fibrosis and sclerosis.
There are no immune complex deposits associated with focal segmental glomerulosclerosis (FSGS).
Treatment of focal segmental glomerulosclerosis (FSGS) is steroids.
If focal segmental glomerulosclerosis (FSGS) does not respond to steroid treatment that portends to a worse diagnosis.
Chronic renal failure is a complication of focal segmental glomerulosclerosis (FSGS).
 Focal Segmental Glomerulosclerosis. High magnification micrograph of focal segmental glomerulosclerosis, hilar variant. Focal segmental glomerulosclerosis is commonly abbreviated FSGS. PAS stain. Kidney biopsy. It presents as a nephrotic syndrome. Related images Intermed. mag. High mag. Very high mag. Nephron - Not altered. CC BY-SA 3.0
Focal Segmental Glomerulosclerosis. High magnification micrograph of focal segmental glomerulosclerosis, hilar variant. Focal segmental glomerulosclerosis is commonly abbreviated FSGS. PAS stain. Kidney biopsy. It presents as a nephrotic syndrome. Related images Intermed. mag. High mag. Very high mag. Nephron - Not altered. CC BY-SA 3.0


Membranous Nephropathy
Membranous nephropathy is the most common cause of nephrotic syndrome in Caucasian adults.
Membranous nephropathy is normally idiopathic.
Known causes of membranous nephropathy include:
- Hepatitis B
- Hepatitis C
- Cancer
- Systemic lupus erythematous (SLE)
- Non-steroidal anti-inflammatory drugs (NSAIDs)
- Penicillamine
- Systemic lupus erythematous
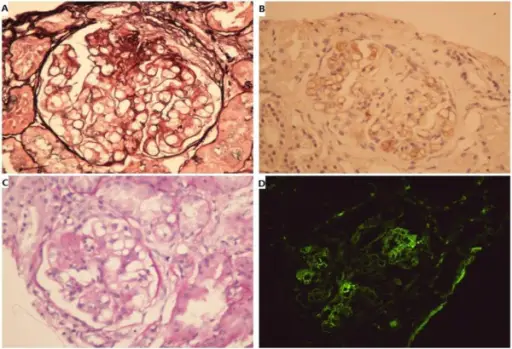
Histology of membranous nephropathy shows glomerular basement membrane thickening.
A periodic acid Schiff (PAS) stain may highlight the thickened basement membrane dark pink.
Electron microscopy of membranous nephropathy shows subepithelial deposits with spike and dome appearance due to immune complex deposition.
Chronic renal failure may develop as a complication of membranous nephropathy.
 Membranous Nephropathy. Very high magnification micrograph of membranous nephropathy, abbreviated MN. MN may also be referred to as membranous glomerulonephritis, abbreviated MGN. Kidney biopsy. Jones stain. The characteristic feature on light microscopy is basement membrane thickening/spike formation, which is best seen with silver stains. On electron microscopy, subepithelial deposits are seen. Related images Intermed. mag. MPAS. High mag. MPAS. Very high mag. MPAS. Very high mag. MPAS. Very high mag. MPAS. (cropped) High mag. HE. Very high mag. HE. Very high mag. PAS. Nephron. Not altered.CC BY-SA 3.0
Membranous Nephropathy. Very high magnification micrograph of membranous nephropathy, abbreviated MN. MN may also be referred to as membranous glomerulonephritis, abbreviated MGN. Kidney biopsy. Jones stain. The characteristic feature on light microscopy is basement membrane thickening/spike formation, which is best seen with silver stains. On electron microscopy, subepithelial deposits are seen. Related images Intermed. mag. MPAS. High mag. MPAS. Very high mag. MPAS. Very high mag. MPAS. Very high mag. MPAS. (cropped) High mag. HE. Very high mag. HE. Very high mag. PAS. Nephron. Not altered.CC BY-SA 3.0


Membranoproliferative Glomerulonephritis (MPGN)
Membranoproliferative glomerulonephritis (MPGN) classically shows a thick glomerular basement membrane on H&E that looks like a “tram-track.”
The tram track appearance of membranoproliferative glomerulonephritis (MPGN) is present because immune complex deposition.
Immunofluorescence of membranoproliferative glomerulonephritis (MPGN) shows immune complex deposition.
The immune complex deposition of membranoproliferative glomerulonephritis (MPGN) is classified into two types based on the location of deposits:
- Type 1 subendothelial (associated with HBV and HCV)
- Type 2 dense deposit disease (which is intramembranous associated with C3 nephritic factor)
Membranoproliferative glomerulonephritis (MPGN) may progress to chronic renal failure.
 Membranoproliferative Glomerulonephritis. Very high magnification micrograph of membranoproliferative glomerulonephritis, abbreviated MPGN. PAS stain. Kidney biopsy. The most common cause of MPGN is hepatitis C. Related images Intermed. mag. High mag. Very high mag. Nephron. Not altered. CC BY-SA 3.0
Membranoproliferative Glomerulonephritis. Very high magnification micrograph of membranoproliferative glomerulonephritis, abbreviated MPGN. PAS stain. Kidney biopsy. The most common cause of MPGN is hepatitis C. Related images Intermed. mag. High mag. Very high mag. Nephron. Not altered. CC BY-SA 3.0


Diabetes Mellitus
High serum glucose levels in patients with diabetes mellitus causes the vascular basement membrane to be glycosylated non-enzymatically, which results in hyaline arteriolosclerosis.
The glomerular efferent arteriole is more impacted than afferent arteriole, resulting in increased glomerular filtration pressure.
Hyperfiltration injury may result in microalbuminuria and nephrotic syndrome.
Diabetes mellitus causes cirrhosis of the mesangium with formation of Kimmelstiel-Wilson nodules.
Diabetes mellitus induced hyaline arteriolosclerosis is treated with angiotensin converting enzyme (ACE) inhibitors.
 Diabetes Mellitus. Retinopathy, nephropathy, and neuropathy are potential complications of diabetes. Complications of Diabetes (from LtoR): Retinopathy, Nephropathy and Neuropathy. Not altered. CC BY-SA 4.0
Diabetes Mellitus. Retinopathy, nephropathy, and neuropathy are potential complications of diabetes. Complications of Diabetes (from LtoR): Retinopathy, Nephropathy and Neuropathy. Not altered. CC BY-SA 4.0
Systemic Amyloidosis
The kidney is the organ that is most often involved by systemic amyloidosis.
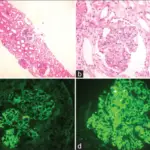
Systemic amyloidosis is characterized by deposits in the mesangium which can cause nephrotic syndrome.
 Systemic Amyloidosis. Amyloidosis, dystrophic calcification Ed Uthman, MD. Not altered. CC BY-SA 2.0
Systemic Amyloidosis. Amyloidosis, dystrophic calcification Ed Uthman, MD. Not altered. CC BY-SA 2.0