Parathyroid Gland Pathology Video
Parathyroid Glands
The parathyroid glands secrete parathyroid hormone (PTH).
Parathyroid hormone (PTH):
- Boosts bone osteoclast activity and releases calcium and phosphate into the serum
- Improves calcium and phosphate absorption in the small intestine by indirectly activating vitamin D
- Leads to elevated serum ionized calcium levels, which acts as a negative feedback to reduce PTH secretion, while decreasing phosphate reabsorption (proximal tubule) and increasing renal calcium reabsorption (distal tubule)
 The parathyroid is well delineated but has a central scar; there is hemorrhage and focal cystic change (top left). The tumor is intensely positive for Bcl-2 (top middle). Nuclear parafibromin is intact (top right). Staining identifies Rb in tumor cell nuclei (bottom left). Galectin-3 is not seen in tumor cells; endothelial cells provide an internal positive control (bottom middle). Cyclin D1 is expressed by the majority of the tumor cell nuclei (bottom right). The dangers of parathyroid biopsy: Neck Surgery. Not altered. CC.
The parathyroid is well delineated but has a central scar; there is hemorrhage and focal cystic change (top left). The tumor is intensely positive for Bcl-2 (top middle). Nuclear parafibromin is intact (top right). Staining identifies Rb in tumor cell nuclei (bottom left). Galectin-3 is not seen in tumor cells; endothelial cells provide an internal positive control (bottom middle). Cyclin D1 is expressed by the majority of the tumor cell nuclei (bottom right). The dangers of parathyroid biopsy: Neck Surgery. Not altered. CC.
Primary Hyperparathyroidism
A disorder of the parathyroid gland itself causes primary hyperparathyroidism, which is characterized by excess parathyroid hormone (PTH).
Causes of primary hyperparathyroidism include:
- Parathyroid adenoma is the most frequent cause, accounting for more than 80% of cases
- Sporadic parathyroid hyperplasia
- Parathyroid cancer
Although primary hyperparathyroidism usually causes asymptomatic hypercalcemia, it can also manifest as a condition with elevated parathyroid hormone (PTH) and hypercalcemia, such as nephrolithiasis or nephrocalcinosis.
Nephrolithiasis is kidney stones.
Nephrocalcinosis may occur due to renal tubule metastatic calcification, perhaps causing renal insufficiency and polyuria.
Symptoms of primary hyperparathyroidism may include:
- Central nervous system (CNS) disturbances
- Depression
- Seizures
- Constipation
- Peptic ulcer disease
- Acute pancreatitis
- Osteitis fibrosa cystica
Osteitis fibrosa cystica is bone resorption resulting in cystic spaces and fibrosis.
Laboratory findings of primary hyperparathyroidism include:
- Increased serum parathyroid hormone (PTH)
- Increased serum calcium
- Decreased serum phosphate
- Increased urinary cAMP
- Increased serum alkaline phosphatase
The afflicted gland is surgically removed as part of treatment.
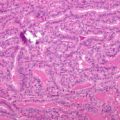
 Histopathological findings of parathyroid adenoma in patients (control) with primary hyperparathyroidism without hyperparathyroidism-induced hypercalcemic crisis (HIHC), (a) Adenoma: Microphotograph showing absence of microcystic pattern, intracytoplasmic vacuoles, and intraglandular fibrosis (H and E, ×100 magnification), (b) Adenoma with capsule: Microphotograph showing thin capsule of parathyroid adenoma. There is absence of microcystic pattern, intracytoplasmic vacuoles, and intraglandular fibrosis (H and E, ×100 magnification). Primary hyperparathyroidism presenting as hypercalcemic crisis: Twenty-year experience. Singh DN, Gupta SK, Kumari N, Krishnani N, Chand G, Mishra A, Agarwal G, Verma AK, Mishra SK, Agarwal A - Indian journal of endocrinology and metabolism (2015 Jan-Feb). Not Altered. CC.
Histopathological findings of parathyroid adenoma in patients (control) with primary hyperparathyroidism without hyperparathyroidism-induced hypercalcemic crisis (HIHC), (a) Adenoma: Microphotograph showing absence of microcystic pattern, intracytoplasmic vacuoles, and intraglandular fibrosis (H and E, ×100 magnification), (b) Adenoma with capsule: Microphotograph showing thin capsule of parathyroid adenoma. There is absence of microcystic pattern, intracytoplasmic vacuoles, and intraglandular fibrosis (H and E, ×100 magnification). Primary hyperparathyroidism presenting as hypercalcemic crisis: Twenty-year experience. Singh DN, Gupta SK, Kumari N, Krishnani N, Chand G, Mishra A, Agarwal G, Verma AK, Mishra SK, Agarwal A - Indian journal of endocrinology and metabolism (2015 Jan-Feb). Not Altered. CC.
Secondary Hyperparathyroidism
Secondary hyperparathyroidism is a condition wherein there is an excess production of parathyroid hormone (PTH) due to a disease process extrinsic to the parathyroid gland.
Chronic renal failure is the most common cause of secondary hyperparathyroidism.
Renal insufficiency leads to decreased phosphate excretion.
Increased serum phosphate binds free calcium.
Free calcium stimulates all four parathyroid glands.
Increased parathyroid hormone (PTH) leads to bone resorption (contributing to renal osteodystrophy).
Laboratory tests of secondary hyperparathyroidism include:
- Increased serum calcium
- Increased serum phosphate
- Increased alkaline phosphatase
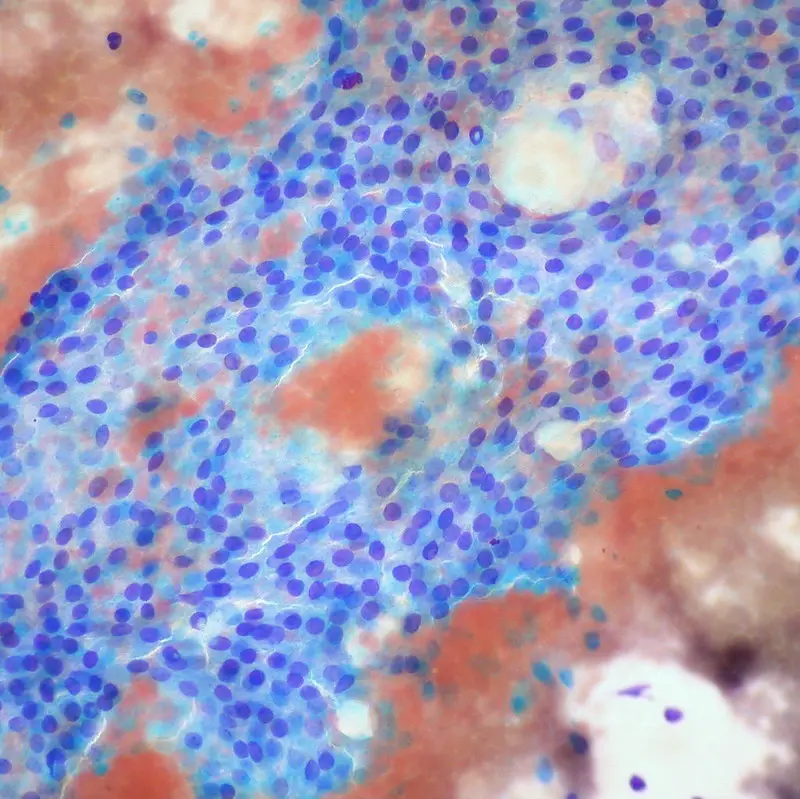
 Parathyroid Gland Pathology. Parathyroid tumor capsule surrounding the soft tissue, 20x magnification. An Interesting Case of Life-Threatening Hypercalcemia Secondary to Atypical Parathyroid Adenoma versus Parathyroid Carcinoma: Mishra A, Newman D - Case reports in medicine (2014). Not altered. CC.
Parathyroid Gland Pathology. Parathyroid tumor capsule surrounding the soft tissue, 20x magnification. An Interesting Case of Life-Threatening Hypercalcemia Secondary to Atypical Parathyroid Adenoma versus Parathyroid Carcinoma: Mishra A, Newman D - Case reports in medicine (2014). Not altered. CC.
Hypoparathyroidism
Hypoparathyroidism causes the body to produce abnormally low levels of the parathyroid hormone (PTH).
Causes of hypothyroidism include:
- Autoimmune damage to the parathyroids
- Surgery
- DiGeorge syndrome
Symptoms of hypothyroidism include:
- Muscle spasms (tetany)
- Chvostek sign may be induced by tapping on the facial nerve (Chvostek sign)
- Trousseau sign filling of the blood pressure cuff
- Numbness
- Tingling
Laboratory tests of hypothyroidism show:
- Decreased parathyroid hormone (PTH) levels
- Decreased serum calcium
 Hypoparathyroidism. Brain computed tomography shows diffuse symmetric parenchymal calcifications involving the cerebellar dentate nuclei (A), basal ganglia (B), and periventricular white matter (C). Widespread intracranial calcifications in a patient with hypoparathyroidism: Seo JY, Seo JH, Choe Y, Seok H, Sohn TS - The Korean journal of internal medicine (2016). Not altered. CC.
Hypoparathyroidism. Brain computed tomography shows diffuse symmetric parenchymal calcifications involving the cerebellar dentate nuclei (A), basal ganglia (B), and periventricular white matter (C). Widespread intracranial calcifications in a patient with hypoparathyroidism: Seo JY, Seo JH, Choe Y, Seok H, Sohn TS - The Korean journal of internal medicine (2016). Not altered. CC.
Pseudohypoparathyroidism
The cause of pseudohypoparathyroidism is end-organ parathyroid hormone (PTH) resistance.
Laboratory tests of pseudohypoparathyroidism reveal:
- Hypocalcemia
- Increased parathyroid hormone (PTH) levels
Short stature and short fourth and fifth digits are characteristics of the autosomal dominant form.