Secondary Hemostasis
Secondary Hemostasis Pathology Video
The whole point of secondary hemostasis is to stabilize the platelet plug.
The main end product of the coagulation cascade is thrombin.
Secondary hemostasis utilizes the coagulation cascade to stabilize the frail platelet plug.
The fibrinogen in the platelet plug is converted to fibrin by the thrombin produced by the coagulation cascade.
The result is a stable platelet-fibrin thrombus when fibrin is cross-linked.
The liver produces coagulation cascade factors.
Certain coagulation cascade factors require potassium, which include:
- Factor 2
- Factor 7
- Factor 9
- Factor 10
Protein C and protein S are also dependent on vitamin K, but these proteins facilitate platelet breakdown and promote bleeding.
Activation of the coagulation cascade requires:
- Exposure to activating substance
- Tissue thromboplastin activates factor V (extrinsic pathway)
- Subendothelial collagen activates factor X (intrinsic pathway)
- Phospholipid surface of platelets
- Calcium (derived from platelet dense granules)
 Secondary Hemostasis. Coagulation with arrows for negative and positive feedback. Joe D. Not altered. CC BY-SA 3.0
Secondary Hemostasis. Coagulation with arrows for negative and positive feedback. Joe D. Not altered. CC BY-SA 3.0


Disorders of Secondary Hemostasis
Disorders of secondary hemostasis are typically the result of an aberrant coagulation factor.
Clinical features of disorders of secondary hemostasis include:
- Deep tissue bleeding into muscles
- Bleeding in joints (hemarthrosis)
- Prolonged bleeding after minor traumas
- Prolonged bleeding after surgery
Laboratory studies used to assess disorders of secondary hemostasis include:
- Prothrombin time (PT)
- Partial thromboplastin time (PTT)
- Bleeding time
- Mixing studies
Prothrombin time (PT) measures extrinsic (factor I) and common (factors V, X, and fibrinogen) pathways of the coagulation cascade.
Partial thromboplastin time (PTT) measures intrinsic (factors X, Xl, IX, VI) and common (factors Il, V, X, and fibrinogen) pathways of the coagulation cascade.
Bleeding time measures the time it takes for bleeding to stop.
Mixing studies check for missing clotting factors.
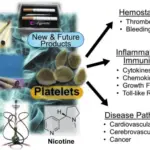
 An overview of important interactions between hemostasis and breast cancer. (1) Hypoxia and oncogenic activation increase tissue factor expression, which increases urokinase-type plasminogen activator (uPA) expression and transcription in tumor cells, facilitating intravasation. (2) Tumor cell-induced platelet aggregation leads to platelet activation. Activated platelets subsequently shed microparticles, release various growth mediators, and protect tumor cells from immune-mediated destruction in circulation. (3) Platelets help in adhesion of tumor cells through p-selectin and integrins, aiding in extravasation from the circulation. (4) Thrombin generated through TF-FVIIa-Xa pathway upregulates growth-related oncogene-alpha (GRO-a) and leads to secretion of matrix metalloproteinase (MMP) and angiogenic molecules. (5) Tissue factor, platelets, thrombin, and the plasminogen system enhance tumor growth, invasion, and angiogenesis, leading to clonogenic accumulation of tumor cells outside breast tissue. FVIIa, activated factor VII; TF, tissue factor. Platelets, coagulation and fibrinolysis in breast cancer progression. Lal I, Dittus K, Holmes CE - Breast cancer research : BCR (2013). Not Altered. CC.
An overview of important interactions between hemostasis and breast cancer. (1) Hypoxia and oncogenic activation increase tissue factor expression, which increases urokinase-type plasminogen activator (uPA) expression and transcription in tumor cells, facilitating intravasation. (2) Tumor cell-induced platelet aggregation leads to platelet activation. Activated platelets subsequently shed microparticles, release various growth mediators, and protect tumor cells from immune-mediated destruction in circulation. (3) Platelets help in adhesion of tumor cells through p-selectin and integrins, aiding in extravasation from the circulation. (4) Thrombin generated through TF-FVIIa-Xa pathway upregulates growth-related oncogene-alpha (GRO-a) and leads to secretion of matrix metalloproteinase (MMP) and angiogenic molecules. (5) Tissue factor, platelets, thrombin, and the plasminogen system enhance tumor growth, invasion, and angiogenesis, leading to clonogenic accumulation of tumor cells outside breast tissue. FVIIa, activated factor VII; TF, tissue factor. Platelets, coagulation and fibrinolysis in breast cancer progression. Lal I, Dittus K, Holmes CE - Breast cancer research : BCR (2013). Not Altered. CC.
Hemophilia A
Hemophilia A is a condition that results in excess bleeding.
Hemophilia A is due to a genetic factor VIIII deficiency.
Hemophilia A is X-linked recessive, which is why it predominantly affects men.
Hemophilia A may occur as a result of a novel mutation (de novo), without any prior family history.
Common symptoms of hemophilia A include:
- Hemarthrosis
- Postsurgical bleeding
The degree of the insufficiency determines the clinical severity.
Laboratory findings of hemophilia A include:
- Increased PTT
- Increased bleeding time
- Normal PT
- Normal platelet count
- Diminished or absent factor VIII levels
In mixing study, factor VIII corrects clot formation.
Hemophilia A is treated with recombinant factor VIII.
 Hemophilia A. Haemarthrosis on lateral view. Nevit Dilmen Hemarthrosis Medical X-rays. Not altered. CC BY-SA 3.0
Hemophilia A. Haemarthrosis on lateral view. Nevit Dilmen Hemarthrosis Medical X-rays. Not altered. CC BY-SA 3.0



Hemophilia B (Christmas Disease)
Hemophilia B is a condition that results in excess bleeding.
Hemophilia B is due to a genetic factor IX deficiency.
Hemophilia B has symptoms and labs similar to hemophilia A, except factor VIII is normal in Hemophilia B.
Factor IX is diminished or absent in hemophilia B.
In mixing study, factor IX corrects hemophilia B.
Hemophilia B is treated with factor IX.
 The patient on presentation with unilateral left cheek swelling. Facial and Scalp Swelling in the Pediatric Population With Hemophilia: A Diagnosis Pitfall. Widjaja W, Aggarwala S, Ballieux F, Vandervord J - Eplasty (2016). Not Altered. CC.
The patient on presentation with unilateral left cheek swelling. Facial and Scalp Swelling in the Pediatric Population With Hemophilia: A Diagnosis Pitfall. Widjaja W, Aggarwala S, Ballieux F, Vandervord J - Eplasty (2016). Not Altered. CC.


Coagulation Factor Inhibitor
There may be acquired antibody production that affects the function of a coagulation factor.
The most common coagulation factor inhibitor is anti-factor VIII.
Anti-factor VIII has the same clinical and lab findings as hemophilia A except the mixing study results.
In anti-factor VIII, due to an inhibitor being present, PTT does not correct when a patient’s plasma is mixed with normal plasma in a mixing study.
 Comparison of FXII−/− and FXI−/− mice in the tMCAO model. (A) Representative TTC-stained coronal sections of FXI−/− and WT mice. Infarct volumes were assessed 24 h after tMCAO (WT, n = 18 and FXI−/−, n = 11; *P < 0.05). (B) Accumulation of fibrin in the infarcted (+) and contralateral (−) hemispheres of WT, FXI−/−, and FXII−/− mice. Fibrin formation 24 h after ischemia was analyzed by immunoblotting using the fibrin-specific antibody 59D8. (C) Immunohistochemical colocalization of fibrin (59D8 antibody) and platelets (anti-GP Ib antibody) in the lumens of microvessels after 24 h in the infarcted hemisphere of WT mice. Bar, 100 μm. (D) Hematoxylin and eosin–stained sections of corresponding territories in the ischemic hemispheres of WT, FXI−/−, and FXII−/− mice. The dark arrows indicate blood vessels that are shown magnified in the inserts. Note the reduced microvascular patency in the ischemic areas of WT animals compared with FXI−/− and FXII−/− mice. Bar, 25 μm. The asterisk denotes the ischemic lesion. Targeting coagulation factor XII provides protection from pathological thrombosis in cerebral ischemia without interfering with hemostasis. Kleinschnitz C, Stoll G, Bendszus M, Schuh K, Pauer HU, Burfeind P, Renné C, Gailani D, Nieswandt B, Renné T - The Journal of experimental medicine (2006). Not Altered. CC.
Comparison of FXII−/− and FXI−/− mice in the tMCAO model. (A) Representative TTC-stained coronal sections of FXI−/− and WT mice. Infarct volumes were assessed 24 h after tMCAO (WT, n = 18 and FXI−/−, n = 11; *P < 0.05). (B) Accumulation of fibrin in the infarcted (+) and contralateral (−) hemispheres of WT, FXI−/−, and FXII−/− mice. Fibrin formation 24 h after ischemia was analyzed by immunoblotting using the fibrin-specific antibody 59D8. (C) Immunohistochemical colocalization of fibrin (59D8 antibody) and platelets (anti-GP Ib antibody) in the lumens of microvessels after 24 h in the infarcted hemisphere of WT mice. Bar, 100 μm. (D) Hematoxylin and eosin–stained sections of corresponding territories in the ischemic hemispheres of WT, FXI−/−, and FXII−/− mice. The dark arrows indicate blood vessels that are shown magnified in the inserts. Note the reduced microvascular patency in the ischemic areas of WT animals compared with FXI−/− and FXII−/− mice. Bar, 25 μm. The asterisk denotes the ischemic lesion. Targeting coagulation factor XII provides protection from pathological thrombosis in cerebral ischemia without interfering with hemostasis. Kleinschnitz C, Stoll G, Bendszus M, Schuh K, Pauer HU, Burfeind P, Renné C, Gailani D, Nieswandt B, Renné T - The Journal of experimental medicine (2006). Not Altered. CC.
Von Willebrand Disease
Von Willebrand disease is a condition that results in excess bleeding.
Von Willebrand disease is due to a genetic von Willebrand factor (VWF) deficiency.
Von Willebrand disease is the most prevalent hereditary coagulation disease.
There are numerous subtypes of Von Willebrand disease that result in both quantitative and qualitative abnormalities.
The autosomal dominant type of Von Willebrand disease, which has lower VWF levels, is the most prevalent type.
Moderate mucosal and cutaneous bleeding is the initial symptom.
There is poor platelet adhesion caused by low von Willebrand factor (VWF).
Laboratory findings include:
- Increased bleeding time
- Normal PTT
- Normal PT
- Normal platelet count
An aberrant ristocetin test is one in which there is no von Willebrand factor (VWF), which results in platelet aggregation being induced by ristocetin.
Desmopressin is used as treatment to promote the release of von Willebrand factor (VWF) from endothelial cells’ Weibel-Palade bodies.
Desmopressin is an anti-diuretic hormone (ADH) analog.
 Von Willebrand Disease. von Willebrand disease type III (and sometimes II) is inherited in an autosomal recessive pattern. C. Burnett - Not altered. CC BY-SA 3.0
Von Willebrand Disease. von Willebrand disease type III (and sometimes II) is inherited in an autosomal recessive pattern. C. Burnett - Not altered. CC BY-SA 3.0






Vitamin K Deficiency
Vitamin K is needed for the production of several components involved with coagulation.
Vitamin K deficiency results in abnormal coagulation factor production of certain coagulation factors.
Coagulation components effected by vitamin K deficiency include:
- Factor 2
- Factor 7
- Factor 9
- Factor 10
- Protein C
- Protein S
Gamma carboxylation is required for the aforementioned factors to function.
Vitamin K gets activated by epoxide reductase which is present in the liver.
All newborn babies receive a prophylactic vitamin K injection at birth to guard against hemorrhagic illness.
Due to lack of gastrointestinal colonization by bacteria that normally manufacture vitamin K, deficiencies can be noted in infants.
Keep in mind that gastrointestinal tract bacteria that produce vitamin K may be disrupted by long-term antibiotic therapy.
Malabsorption may also cause a lack of fat-soluble vitamins, such as vitamin K, leading to clotting issues.
 Multiple nodular lesions on right elbow, right knee, and lateral side of chest (Highlighted by black arrows). Vitamin k deficiency bleeding presenting as nodular purpura in infancy: a rare and life-threatening entity. Gahalaut P, Chauhan S - Indian journal of dermatology (2013). Not Altered. CC.
Multiple nodular lesions on right elbow, right knee, and lateral side of chest (Highlighted by black arrows). Vitamin k deficiency bleeding presenting as nodular purpura in infancy: a rare and life-threatening entity. Gahalaut P, Chauhan S - Indian journal of dermatology (2013). Not Altered. CC.
Other Issues of Abnormal Secondary Hemostasis
The effect of liver failure on coagulation is monitored by PT.
Liver failure can result in decreased synthesis of coagulation factors and decreased activation of vitamin K by epoxide reductase.
Large volume transfusions can dilute the coagulation factors, which may cause a relative shortage of coagulation factors.