Skin
The skin serves as a defense against fluid loss and environmental irritants.
Skin is made up of a dermis and an epidermis.
The epidermis is composed of keratinocytes and has five layers:
- Basale
- Spinosum
- Granulosum
- Lucidum
- Corneum
The regenerative stem cell layer is found in the stratum basalis.
The stratum spinosum is also distinguished by desmosomes between keratinocytes.
The stratum granulosum is distinguished by granules in keratinocytes.
The stratum lucidum is smooth and translucent.
The stratum corneum is distinguished by keratin in anucleate cells.
The dermis is made up of connective tissue, nerve endings, blood and lymphatic arteries, and adnexal structures such as hair shafts, sweat glands, and sebaceous glands.
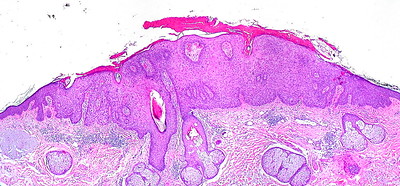
 Lichen Simplex Chronicus. Very low magnification micrograph of lichen simplex chronicus, abbreviated LSC. H&E stain. Skin biopsy. Features: Acanthosis (epidermal thickening). Hyperkeratosis (thickened stratum corneum). Parakeratosis = retention of nuclei in the stratum corneum. +/- Spongiosis (epidermal intercellular edema -- cells appear to have a clear halo around 'em). Nephron. Not altered. CC BY-SA 3.0
Lichen Simplex Chronicus. Very low magnification micrograph of lichen simplex chronicus, abbreviated LSC. H&E stain. Skin biopsy. Features: Acanthosis (epidermal thickening). Hyperkeratosis (thickened stratum corneum). Parakeratosis = retention of nuclei in the stratum corneum. +/- Spongiosis (epidermal intercellular edema -- cells appear to have a clear halo around 'em). Nephron. Not altered. CC BY-SA 3.0

Inflammatory Dermatoses
Atopic Dermatitis
Atopic dermatitis is also known as eczema.
An itchy, erythematous, oozing rash with vesicles and edema is present in atopic dermatitis.
Atopic dermatitis frequently affects the flexor and facial surfaces.
Asthma and allergic rhinitis are connected with a type 1 hypersensitivity reaction and are commonly found in patients with atopic dermatitis.
 Atopic Dermatitis. Atopy of the flexure crease of the elbow. James Heilman, MD. Not altered. CC BY-SA 3.0
Atopic Dermatitis. Atopy of the flexure crease of the elbow. James Heilman, MD. Not altered. CC BY-SA 3.0

Contact Dermatitis
A pruritic, erythematous, oozing rash with vesicles and edema is a hallmark of contact dermatitis.
Contact dermatitis is caused by the skin coming in “contact” with an allergen or irritant, such as:
- Nickel jewelry
- Poison ivy
- Irritant chemicals
- Penicillin
Treatment of contact dermatitis includes:
- Removing the offending agent
- Topical glucocorticoids (if necessary)
 Contact Dermatitis. Contact dermatitis around a healing rugburn. The burn was wrapped in a bandage that the wearer was sensitive to, causing an outbreak of itchy, raised spots. Not altered. Public Domain
Contact Dermatitis. Contact dermatitis around a healing rugburn. The burn was wrapped in a bandage that the wearer was sensitive to, causing an outbreak of itchy, raised spots. Not altered. Public Domain



Acne Vulgaris
Acne vulgaris is characterized by the presence of nodules, pustules, and comedones, such as whiteheads and blackheads.
Acne vulgaris can be caused by persistent inflammation of the sebaceous glands and hair follicles, they are exceedingly frequent, especially in adolescents.
Hormone-associated increase in sebum production where sebaceous glands have androgen receptors and excess keratin production block follicles, forming comedones.
Infection with Propionibacterium acnes results in the production of lipases, which degrade sebum and release proinflammatory fatty acids, causing pustule or nodule growth.
Acne vulgaris can be treated with:
- Benzoyl peroxide, an antibacterial, is used as a treatment
- Vitamin A compounds like isotretinoin that lower keratin synthesis
 Acne Vulgaris. Image of an 18 year old male with moderate acne vulgaris (white heads). His face appears to be very oily as well. Roshu Bangal. Not altered. CC BY-SA 4.0
Acne Vulgaris. Image of an 18 year old male with moderate acne vulgaris (white heads). His face appears to be very oily as well. Roshu Bangal. Not altered. CC BY-SA 4.0






Psoriasis
Psoriasis is characterized by well-circumscribed salmon-colored plaques with silvery scales on extensor surfaces and the scalp.
Nail pitting may also be evident in psoriasis.
Psoriasis is due to excessive keratinocyte proliferation.
There is possibly an autoimmune etiology of psoriasis associated with HLA-C.
Psoriasis is associated with an environmental trigger.
Traumatized skin areas frequently have psoriasis lesions in patients with this condition.
The histology of psoriasis includes:
- Acanthosis or epidermal hyperplasia
- Hyperkeratosis
- Parakeratosis (retention of keratinocyte nuclei in the stratum corneum)
- The Auspitz sign is associated with psoriasis
The Auspitz sign is when scale is picked off, neutrophils in the stratum corneum and thinning of the epidermis above elongated dermal papillae cause bleeding
Psoriasis is treated with:
- Corticosteroids
- Ultraviolet (UV) light with psoralen
- Immune-modulating therapy
 Psoriasis. Plaques of psoriasis. James Heilman, MD. CC BY-SA 3.0
Psoriasis. Plaques of psoriasis. James Heilman, MD. CC BY-SA 3.0










Lichen Planus (LP)
Pruritic, planar, polygonal, purple papules with reticular while lines on their surface describe lichen planus (LP).
Lichen planus (LP) most usually affects the wrists, elbows, and oral mucosa.
Oral involvement in lichen planus (LP) manifests as Wickham striae.
Histology of lichen planus (LP) shows inflammation of the dermal-epidermal junction with a saw-tooth appearance.
Although the etiology of lichen planus (LP) is unknown, it is found to be associated with chronic hepatitis C virus infection.
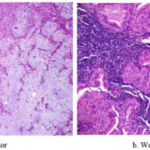
 Lichen Planus. Histopathology of lichen planus. Micrograph of lichen planus. H&E stain. Features: Loss of rete ridges. Loss of basal cells (stratum basale). Interface dermatitis (lymphocytes at dermal-epidermal junction). Related images Low mag. Nephron. CC BY-SA 3.0
Lichen Planus. Histopathology of lichen planus. Micrograph of lichen planus. H&E stain. Features: Loss of rete ridges. Loss of basal cells (stratum basale). Interface dermatitis (lymphocytes at dermal-epidermal junction). Related images Low mag. Nephron. CC BY-SA 3.0







Blistering Dermatoses
Pemphigus Vulgaris PV
Pemphigus vulgaris (PV) is the autoimmune destruction of desmosomes between keratinocytes caused by an antibody against desmoglein (type 1 hypersensitivity) that manifests as skin and oral mucosa bullae.
Pemphigus vulgaris (PV) is characterized by suprabasalar blisters caused by acantholysis, or the separation of stratum spinosum keratinocytes that are ordinarily united by desmosomes.
Hemidesmosomes keep basal layer cells connected to the basement membrane.
Shallow erosions and dry crust result from rapidly rupturing thin-walled bullae.
In pemphigus vulgaris (PV), IgG surrounds keratinocytes in a fishnet-like pattern during immunofluorescence.
 Pemphigus Vulgaris. Intermediate magnification micrograph of pemphigus vulgaris. H&E stain. Related images Low mag. Intermed. mag. High mag. Very high mag. Nephron. Not altered. CC BY-SA 3.0
Pemphigus Vulgaris. Intermediate magnification micrograph of pemphigus vulgaris. H&E stain. Related images Low mag. Intermed. mag. High mag. Very high mag. Nephron. Not altered. CC BY-SA 3.0


Bullous Pemphigoid (BP)
Bullous pemphigoid (BP) is an autoimmune destruction of hemidesmosomes between basal cells and the underlying basement membrane due to lgG antibody against basement membrane collagen.
Bullous pemphigoid (BP) presents as blisters of the skin and oral mucosa is spared.
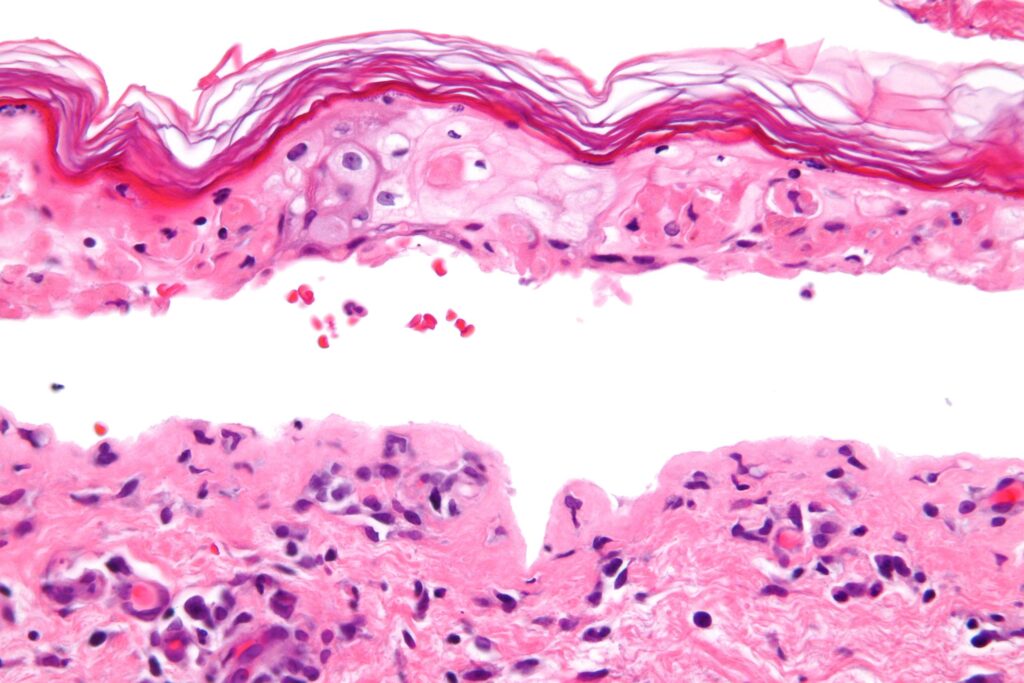
 Bullous Pemphigoid. Micrograph of bullous pemphigoid. Subepidermal blistering [solid arrows in (A,B)] and influx of inflammatory cells including eosinophils and neutrophils in thedermis [solid arrow (C)] and blister cavity [dashed arrows (C)]. In (C) also deposition of fibrin is noted (asterisks). Jenny Giang, Marc A. J. Seelen, Martijn B. A. van Doorn, Robert Rissmann,Errol P. Prens and Jeffrey Damman - (2018). "Complement Activation in Inflammatory Skin Diseases". Frontiers in Immunology 9. DOI:10.3389/fimmu.2018.00639. ISSN 1664-3224. "Figures - available via license: CC BY 4.0"
Bullous Pemphigoid. Micrograph of bullous pemphigoid. Subepidermal blistering [solid arrows in (A,B)] and influx of inflammatory cells including eosinophils and neutrophils in thedermis [solid arrow (C)] and blister cavity [dashed arrows (C)]. In (C) also deposition of fibrin is noted (asterisks). Jenny Giang, Marc A. J. Seelen, Martijn B. A. van Doorn, Robert Rissmann,Errol P. Prens and Jeffrey Damman - (2018). "Complement Activation in Inflammatory Skin Diseases". Frontiers in Immunology 9. DOI:10.3389/fimmu.2018.00639. ISSN 1664-3224. "Figures - available via license: CC BY 4.0"


Dermatitis Herpetiformis
IgA is deposited by the immune system at the ends of dermal papillae in dermatitis herpetiformis (DH).
Dermatitis herpetiformis (DH) lesions appear as clusters of pruritic vesicles and bullae.
Celiac disease has a high correlation with dermatitis herpetiformis (DH) and can be treated with a gluten-free diet.
In this condition, the basal cell layer is detached from the basement membrane.
Tense bullae of dermatitis herpetiformis (DH) are clinically less severe than pemphigus vulgaris (PV) and do not rupture easily.
Immunofluorescence of dermatitis herpetiformis (DH) shows lgG along the basement membrane in a linear pattern.
 Dermatitis Herpetiformis. Characteristic rash resembles herpes and is the basis of its clinical name dermatitis herpetiformis. Thomas Habif. Not altered. CC BY-SA 3.0
Dermatitis Herpetiformis. Characteristic rash resembles herpes and is the basis of its clinical name dermatitis herpetiformis. Thomas Habif. Not altered. CC BY-SA 3.0




Erythema Multiforme (EM)
Targetoid rash and bullae are the hallmarks of the hypersensitive reaction known as erythema multiforme (EM).
The targetoid appearance of erythema multiforme (EM) is caused by erythema surrounding a core epidermal necrosis.
The most common causes of erythema multiforme (EM) include:
- Herpes simplex virus (HSV) infection
- Mycoplasma infection
- Medications (penicillin and sulfonamides)
- Autoimmune disorders
- Malignancy
 Erythema Multiforme. Erythema multiforme minor (note of make of the blanching centers of the lesion). James Heilman, MD. James Heilman, MD. CC BY-SA 3.0
Erythema Multiforme. Erythema multiforme minor (note of make of the blanching centers of the lesion). James Heilman, MD. James Heilman, MD. CC BY-SA 3.0




Stevens-Johnson Syndrome (SJS)
Stevens-Johnson syndrome (SJS), is characterized by erythema multiforme (EM) with oral mucosa/lip involvement, fever, and skin sloughing.
Steven-Johnson syndrome (SJS) is like toxic epidermal necrolysis (TEN).
Steven-Johnson syndrome (SJS) is less than 30% body surface area involvement.
Toxic Epidermal Necrolysis (TEN)
Toxic epidermal necrolysis (TEN) is a severe variant of Stevens-Johnson syndrome (SJS).
Toxic epidermal necrolysis (TEN) greater than 30% body surface area involvement.
The most frequent cause of toxic epidermal necrolysis (TEN) medication reaction.

Epithelial Tumors
Seborrheic Keratosis (SK)
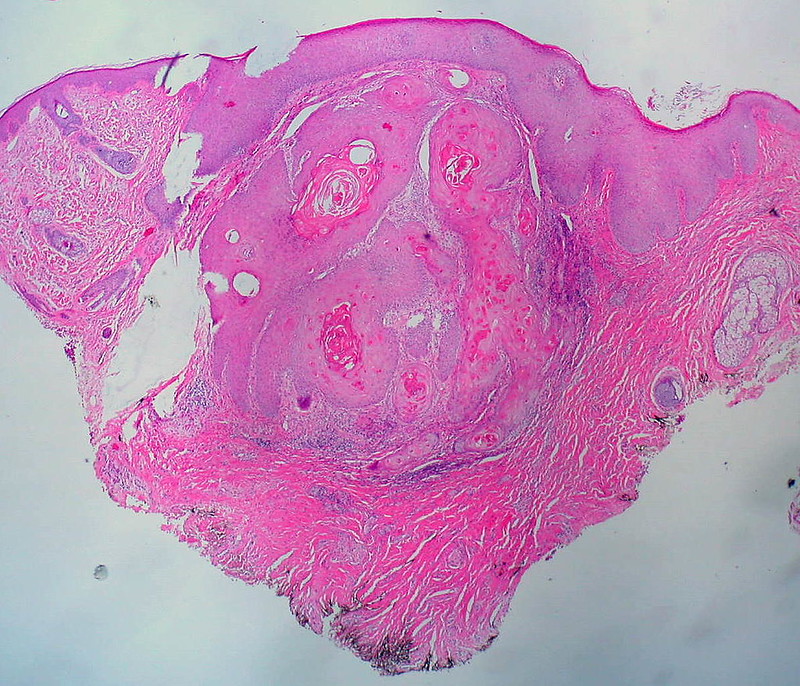
Seborrheic keratosis (SK) is a benign squamous proliferation is thought to be a typical tumor in elderly people.
Seborrheic keratosis (SK) typically appears as elevated, discolored plaques with a coin-like, waxy, stuck-on appearance on the extremities or face.
Seborrheic keratosis (SK) exhibits the histological feature of keratin pseudocysts.
The Leser-Trélat sign, which is the abrupt emergence of numerous seborrheic keratoses (SK) and signals underlying gastrointestinal malignancy.
 Seborrheic Keratosis. Many seborrheic keratosis on the back of a person with Leser–Trélat sign due to colon cancer. James Heilman, MD. CC BY-SA 3.0
Seborrheic Keratosis. Many seborrheic keratosis on the back of a person with Leser–Trélat sign due to colon cancer. James Heilman, MD. CC BY-SA 3.0


Acanthosis Nigricans
Acanthosis nigricans is a condition where there is epidermal hyperplasia and skin darkening that frequently affects the axilla or groin.
Acanthosis nigricans is linked to malignancies, particularly gastric cancer, or insulin resistance, such as non-insulin-dependent diabetes.
 Acanthosis Nigricans. Left axillary involved by acanthosis nigricans. Thomas Habif. Not altered. CC BY-SA 3.0
Acanthosis Nigricans. Left axillary involved by acanthosis nigricans. Thomas Habif. Not altered. CC BY-SA 3.0




Basal Cell Carcinoma (BCC)
Basal cell carcinoma (BCC) is the malignant proliferation of the basal cells of the epidermis.
Basal cell carcinoma (BCC) is the most common cutaneous malignancy.
Long-term sun exposure, albinism, and xeroderma pigmentosum are risk factors that result from DNA damage caused by UVB radiation.
Basal cell carcinoma (BCC) commonly appears as a raised nodule with a pink, pearl-like papule in the center and dilated telangiectatic vessels surrounding it.
Basal cell carcinoma (BCC) is classic located on is the upper lip.
Basal cell nodules (BCC) with peripheral palisading are visible in histology.
Basal cell carcinoma (BCC) rarely metastasizes.
Basal cell carcinoma (BCC) is treated by surgical excision.
 Basal Cell Carcinoma. Basal cell carcinoma on patient's back. Basal cell carcinoma is the most common skin cancer. John Hendrix. Public domain.
Basal Cell Carcinoma. Basal cell carcinoma on patient's back. Basal cell carcinoma is the most common skin cancer. John Hendrix. Public domain.









Squamous Cell Carcinoma (SCC)
Squamous cell carcinoma (SCC) is a malignant proliferation of squamous cells characterized by formation of keratin pearls.
- Risk factors for squamous cell carcinoma (SCC) include:
- Prolonged sun exposure
- Use of tanning beds
- Immunosuppressive medications
- Exposure to arsenic
- Chronic inflammatory conditions including burn scars or nasal drainage
Squamous cell carcinoma (SCC) typically manifests as a nodular, ulcerated mass on the face, typically involving the lower lip.
Treatment of squamous cell carcinoma (SCC) is surgical excision.
 Squamous Cell Carcinoma. Squamous cell carcinoma, left ventral forearm. Dermanonymous. Not altered. CC BY-SA 4.0
Squamous Cell Carcinoma. Squamous cell carcinoma, left ventral forearm. Dermanonymous. Not altered. CC BY-SA 4.0








Actinic Keratosis (AK)
Actinic keratosis (AK) is a precancerous lesion that frequently develops on the face, back, or neck and manifests as a hyperkeratotic, scaly plaque.
Keratoacanthoma
A keratoacanthoma is a benign epithelial tumor with squamous elements.
While keratoacanthoma develops quickly and spontaneously regresses, it is a well-differentiated squamous cell carcinoma that looks like a cup-shaped tumor loaded with keratin debris.
Melanocytic Disorders
Melanocytes are responsible for skin pigmentation and are present in the basal layer of the epidermis.
Melanocytes are derived from the neural crest.
Melanocytes synthesize melanin in melanosomes using tyrosine as a precursor molecule to pass melanin to keratinocytes.
 Melanoma. ABCD rule illustration: On the left side from top to bottom: melanomas showing (A) Asymmetry, (B) a border that is uneven, ragged, or notched, (C) coloring of different shades of brown, black, or tan and (D) diameter that had changed in size. The normal moles on the right side do not have abnormal characteristics (no asymmetry, even border, even color, no change in diameter). Not altered. Public Domain
Melanoma. ABCD rule illustration: On the left side from top to bottom: melanomas showing (A) Asymmetry, (B) a border that is uneven, ragged, or notched, (C) coloring of different shades of brown, black, or tan and (D) diameter that had changed in size. The normal moles on the right side do not have abnormal characteristics (no asymmetry, even border, even color, no change in diameter). Not altered. Public Domain

Vitiligo
The autoimmune death of melanocytes causes vitiligo.
Vitiligo is characterized by localized loss of skin pigmentation.
 Vitiligo. Vitiligo of the hand in a person with dark skin. James Heilman, MD. CC BY-SA 3.0. Not altered. CC.
Vitiligo. Vitiligo of the hand in a person with dark skin. James Heilman, MD. CC BY-SA 3.0. Not altered. CC.






Albinism
Congenital absence of pigmentation caused by a tyrosinase deficiency that hinders melanin formation is known as albinism.
Albinism may involve the eyes (ocular form), or both the skin and eyes (oculocutaneous form).
Reduced ultraviolet B (UVB) protection in albino patients increases the risk of squamous cell carcinoma (SCC), basal cell carcinoma (BCC), and melanoma.
 Albinism. Girl with albinism from Papua New Guinea. Muntuwandi. Not altered. CC BY-SA 3.0
Albinism. Girl with albinism from Papua New Guinea. Muntuwandi. Not altered. CC BY-SA 3.0


Freckles
Freckles are also called ephelis.
Freckles tend to be small, tan to brown, macules.
Freckles darken in the presence of sunlight due to an increase in melanosomes but not melanocytes.
 Freckles. Photograph of two friends who have freckled faces. Are they friends or are they sisters? Are they twins? Are they twins that are friends? You be the judge. Not altered. Public domain.
Freckles. Photograph of two friends who have freckled faces. Are they friends or are they sisters? Are they twins? Are they twins that are friends? You be the judge. Not altered. Public domain.

Melasma
Melasma is a mask-like darkening of the cheeks.
Melasma is associated with:
- Pregnancy
- Oral contraceptives
 Melasma. Melasma on the face. Not altered. CC BY-SA 3.0
Melasma. Melasma on the face. Not altered. CC BY-SA 3.0

Nevus
A nevus is also known as a mole.
Nevi (plural for nevus) are also known as moles.
Nevi are benign neoplasms of melanocytes.
Congenital nevus is present at birth which is often associated with hair and acquired nevus arises later in life.
The most common mole in children, junctional nevi, start as nests of melanocytes at the dermal-epidermal junction.
Compound nevus exist within the junction and the dermis.
The most common mole in adults is an intradermal nevus, which develops when the junctional component eventually disappears.
In general, nevi are characterized by a flat macule or raised papule with symmetry, sharp borders, evenly distributed color, and small diameter (< 6 mm).
Dysplasia may arise and may be called the dysplastic nevus, which is a precursor to melanoma.
 Nevus. National Cancer Institute - Source: National Cancer Institute. Not altered. Public domain.
Nevus. National Cancer Institute - Source: National Cancer Institute. Not altered. Public domain.



















Melanoma
The malignant neoplasm of melanocytes is called melanoma.
This is regarded as the most prevalent reason for skin cancer fatalities.
Risk factors for melanoma include:
Xeroderma pigmentosum
- Albinism
- Norwegian descent
- Chronic sun exposure
- Risk factors are all based on UVB-induced DNA damage of the skin
Dysplastic nevus syndrome, an autosomal dominant condition marked by the development of dysplastic nevi that may lead to melanoma, is another risk factor.
Melanoma can be differentiated form a nevus using the ABCD mnemonic:
- A for asymmetry
- B for irregular borders
- C for color
- D for diameter more than 6 mm.
Melanoma is characterized by two growth phases:
- Radial growth (wide)
- Vertical growth (depth)
While vertical development penetrates the deep dermis, radial growth occurs along the epidermis and superficial dermis with little chance of metastasis.
Melanoma has an increased risk of metastasis; depth of extension or Breslow thickness is the most important prognostic factor in predicting metastasis.
Variants of melanoma include:
- Superficial spreading
- Lentigo maligna
- Nodular
- Acral lentiginous
The most prevalent subtype of melanoma, superficial spreading, is prominent in the early stages of radial expansion and has a favorable prognosis.
Lentiginous proliferation with radial growth characterizes lentigo maligna melanoma, which has a favorable prognosis.
The nodular variant of melanoma has early vertical development and shows poor prognosis.
The palms or soles of people with dark skin frequently develop acral lentiginous melanoma.
 Melanoma. This slide shows a melanoma on a patient's skin. National Cancer Institute. Not altered. Public Domain.
Melanoma. This slide shows a melanoma on a patient's skin. National Cancer Institute. Not altered. Public Domain.


































Infectious Skin Disorders
Impetigo
The superficial bacterial skin infection known as impetigo.
Common causes of impetigo include:
- Stahyloccocus Aureus
- Streptococcus Pyogenes
Impetigo typically presents on the face, as erythematous macules that develop into pustules.
When the pustules of impetigo rupture, erosions dry, and a honey-crust is produced.
 Impetigo. Honey colored crust characteristic of impetigo. James Heilman, MD. Not altered. CC BY-SA 4.0
Impetigo. Honey colored crust characteristic of impetigo. James Heilman, MD. Not altered. CC BY-SA 4.0




Cellulitis
Cellulitis manifests as a red, tender, swollen rash with a fever and is a deeper (dermal and subcutaneous) infection.
Risk factors for cellulitis include:
- Insect bites
- Trauma
- Recent surgery
- Scratching
- Open skin wounds
Common causes of cellulitis include:
- Staphylococcus Aureus
- Streptococcus Pyogenes
Due to an infection with anaerobic flesh-eating bacteria, cellulitis can progress to necrotizing fasciitis with necrosis of subcutaneous tissues.
Production of carbon dioxide (CO2) leads to crepitus.
Cellulitis is a surgical emergency.
 Cellulitis. Cellulitis of left knee. Rafael Lopez. Not altered. CC BY-SA 3.0
Cellulitis. Cellulitis of left knee. Rafael Lopez. Not altered. CC BY-SA 3.0



Staphylococcal Scalded Skin Syndrome
Staphylococcal scalded skin syndrome (SSSS) is characterized by skin sloughing, an erythematous rash, and fever.
Staphylococcal scalded skin syndrome (SSSS) is due to exfoliative A and B toxins that cause epidermolysis of the stratum granulosum.
Staphylococcus Aureus produces exfoliative A and B toxins.
Staphylococcal scalded skin syndrome (SSSS) is distinguished histologically from toxic epidermal necrolysis by the level of skin separation.
In TEN the separation is at the dermal-epidermal junction.
In SSSS the separation is at the stratum granulosum.
 Staphylococcal Scalded Skin Syndrome. Baby clutches fist as skin sloughs off due to Staphylococcal Scalded Skin Syndrome (SSSS). Not altered. CC BY 4.0
Staphylococcal Scalded Skin Syndrome. Baby clutches fist as skin sloughs off due to Staphylococcal Scalded Skin Syndrome (SSSS). Not altered. CC BY 4.0
Verruca
Verrucas are also called warts.
Verrucas, are flesh-colored papules with a rough surface that develop after keratinocytes become infected with the HPV virus and are distinguished by koilocytic alteration.
The hands, feet, and ano-genital region are common locations for verruca.
 Verruca. Two painful plantar warts at the soles of a 16 year old girl. Despite repeated deep curettage they reoccurred again and again, getting more painful after every surgery. Since the last removal, the pain is so extreme that the 16-year-old girl is severely disabled when walking. Węgrowski. Not altered. CC BY-SA 4.0
Verruca. Two painful plantar warts at the soles of a 16 year old girl. Despite repeated deep curettage they reoccurred again and again, getting more painful after every surgery. Since the last removal, the pain is so extreme that the 16-year-old girl is severely disabled when walking. Węgrowski. Not altered. CC BY-SA 4.0









Molluscum Contagiosum
Molluscum contagiosum are hard, pink, umbilicated papules on the skin.
The poxvirus causes molluscum contagiosum.
Cytoplasmic inclusions are visible in affected keratinocytes.
Molluscum contagiosum are most commonly seen in children.
Adults with molluscum contagiosum should be screened for immunocompromising issues (i.e. HIV).
 Molluscum Contagiosum. Molluscum contagiosum, or water wart. Evanherk. Not altered. CC BY-SA 3.0
Molluscum Contagiosum. Molluscum contagiosum, or water wart. Evanherk. Not altered. CC BY-SA 3.0