Valvular Disorders
Valvular Disorders Pathology Video
The heart has four valves:
- Aortic valve
- Pulmonic valve
- Tricuspid valve
- Mitral valve
The cardiac valves ideally prevent backflow.
Valvular lesions generally result in stenosis or regurgitation.
 Valvular Disorders Pathology. Phonocardiograms from normal and abnormal heart sounds Madhero88. Not altered. CC BY-SA 3.
Valvular Disorders Pathology. Phonocardiograms from normal and abnormal heart sounds Madhero88. Not altered. CC BY-SA 3.


Acute Rheumatic Fever
Acute rheumatic fever is caused by group A beta-hemolytic streptococci.
Children are susceptible to this systemic consequence of streptococcal pharyngitis, often known as strep throat, 2 – 3 weeks after an episode.
Acute rheumatic fever is caused by molecular mimicry due to a bacterial M protein that resembles proteins in human tissue.
Diagnosis of acute rheumatic fever is based on the Jones criteria which consist of major and minor criteria.
Major criteria of Jones criteria for diagnosing acute rheumatic fever include:
JONES
J-Joints (arthritis, swollen joints, hot joints)
O-(looks like a “Heart” -> (myocarditis, endocarditis, cardiac valve issues, pericarditis)
N-Nodules (skin nodules on extensor surfaces)
E-Erythema marginatum (a specific type of rash)
S-Sydenham chorea (abnormal movement disorder)
Minor criteria of Jones criteria for diagnosing acute rheumatic fever:
PEACE
P-Previous history of rheumatic fever
E-Echocardiogram (ECG) with PR prolongation
A-Arthralgias
C-CRP elevated
E-Elevated erythrocyte sedimentation rate (ESR) and temperature (fever)
Prior evidence of a group A beta-hemolytic streptococcus infection aids with the diagnosis as well.
Specific labs that will aid in the diagnosis of acute rheumatic fever include:
- Antistreptolysin O (ASO) titer
- Anti-DNase B titer
Diagnosis of acute rheumatic fever require two major and one minor features being present or one major and two minor features being present.
The mitral valve is the most affected cardiac valve.
Small vegetations accrue on the valve along the lines of closure that result in mitral regurgitation.
Histology classically shows reactive histiocytes with slender, wavy nuclei are known as Anitschkow cells, Aschoff bodies, gigantic cells, and fibrinoid material.
The most frequent cause of death in acute rheumatic fever is myocarditis.
Erythema marginatum is a non-pruritic annular rash with erythematous borders that often affects the trunk and limbs.
Pericarditis causes friction rub and chest pain.
Sydenham chorea is the rapid, involuntary muscle movements.
The acute attack normally goes away, but it could turn into a persistent case of rheumatic heart disease.
Relapse of the acute phase and increased risk for chronic disease are brought on by repeated exposure to group A hemolytic streptococci.
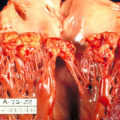
 Acute Rheumatic Fever. Source says: "Gross pathology of rheumatic heart disease. Left ventricle has been cut open to display characteristic severe thickening of mitral valve, thickened chordae tendineae, and hypertrophied left ventricular myocardium. Autopsy." CDC/Dr. Edwin P. Ewing, Jr. - Public Health Image Library (PHIL) ID#: 847. Not altered. Public Domain
Acute Rheumatic Fever. Source says: "Gross pathology of rheumatic heart disease. Left ventricle has been cut open to display characteristic severe thickening of mitral valve, thickened chordae tendineae, and hypertrophied left ventricular myocardium. Autopsy." CDC/Dr. Edwin P. Ewing, Jr. - Public Health Image Library (PHIL) ID#: 847. Not altered. Public Domain


Chronic Rheumatic Heart Disease
Chronic rheumatic heart disease develops when rheumatic fever-related valve scarring leads to stenosis with the classic fish-mouth appearance.
In chronic rheumatic heart disease, the chordae tendineae and cusps thicken as a result of the mitral valve being involved almost always.
Quite often the aortic valve is involved, which results in the commissures fusing together.
Other valves are less commonly involved and complications include infectious endocarditis.
 Histologic and immunohistochemical findings of the rheumatic mitral valves. (A) Rheumatic mitral valves showed severe fibrosis and distorted architecture (H&E, ×40). (B) A high-power view demonstrated small thin-walled vessels and perivascular lymphocytic infiltration (H&E, ×200). (C) High TGF-β1 expression was seen in the endothelial cells and smooth muscle cells of the vessels, in the perivascular interstitial cells, and stroma of the valves (×200). (D) Myofibroblasts that were positive for SMA immunostaining were present in the subendothelial densely fibrotic area (×40). Overexpression of transforming growth factor-beta 1 in the valvular fibrosis of chronic rheumatic heart disease. Kim L, Kim do K, Yang WI, Shin DH, Jung IM, Park HK, Chang BC - Journal of Korean medical science (2008). Not Altered. CC.
Histologic and immunohistochemical findings of the rheumatic mitral valves. (A) Rheumatic mitral valves showed severe fibrosis and distorted architecture (H&E, ×40). (B) A high-power view demonstrated small thin-walled vessels and perivascular lymphocytic infiltration (H&E, ×200). (C) High TGF-β1 expression was seen in the endothelial cells and smooth muscle cells of the vessels, in the perivascular interstitial cells, and stroma of the valves (×200). (D) Myofibroblasts that were positive for SMA immunostaining were present in the subendothelial densely fibrotic area (×40). Overexpression of transforming growth factor-beta 1 in the valvular fibrosis of chronic rheumatic heart disease. Kim L, Kim do K, Yang WI, Shin DH, Jung IM, Park HK, Chang BC - Journal of Korean medical science (2008). Not Altered. CC.


Aortic Stenosis
Aortic stenosis occurs when the aortic valve orifice narrows.
Aortic stenosis is typically brought on by fibrosis and calcification from wear and tear.
Aortic stenosis usually effects individuals above 60-years-old.
Risk factors for developing aortic stenosis include:
- Having a bicuspid aortic valve
- Rheumatic valve disease
Aortic stenosis causes a crescendo-decrescendo murmur after a systolic ejection click.
Complications of aortic stenosis include:
- Concentric left ventricular hypertrophy
- Angina
- Syncope
- Cardiac failure
- Microangiopathic hemolytic anemia
Treatment of aortic stenosis is valve replacement.
 Aortic stenosis. Gross pathology of rheumatic heart disease: aortic stenosis. Aorta has been removed to show thickened, fused aortic valve leaflets and opened coronary arteries from above. Autopsy. CDC/Dr. Edwin P. Ewing, Jr. Not altered. Public Domain
Aortic stenosis. Gross pathology of rheumatic heart disease: aortic stenosis. Aorta has been removed to show thickened, fused aortic valve leaflets and opened coronary arteries from above. Autopsy. CDC/Dr. Edwin P. Ewing, Jr. Not altered. Public Domain



Aortic Regurgitation
Aortic regurgitation is the backflow of blood from the aorta into the left ventricle during diastole caused by aortic root dilatation or valve damage.
Aortic regurgitation is the most common cause of isolated aortic root dilation.
Clinical features of aortic regurgitation include an early, blowing diastolic murmur and hyperdynamic circulation due to increased pulse pressure.
The difference between systolic and diastolic pressures is known as pulse pressure.
Diastolic pressure decreases as a result of regurgitation, but systolic pressure increases as a result of increased stroke volume.
The increased pulse pressure associated with aortic regurgitation is characterized by:
- Water-hammer pulse
- Pulsating nail bed also known as the Quincke pulse
- Head bobbing
Aortic regurgitation results in left ventricle dilation and eccentric hypertrophy due to volume overload.
Treatment of aortic regurgitation is valve replacement once left ventricle dysfunction develops.
 Aortic Regurgitation. Aortic Regurgitation. See a related animation of this medical topic. Bruce Blaus. Not altered. CC BY 3.0
Aortic Regurgitation. Aortic Regurgitation. See a related animation of this medical topic. Bruce Blaus. Not altered. CC BY 3.0


Mitral Valve Prolapse
Mitral valve prolapse is the ballooning of the mitral valve into the left atrium during systole.
Mitral valve prolapse is present in 2 – 3% of American adults due to myxoid degeneration of the mitral valve, which causes it to become floppy.
The cause of mitral valve prolapse is unknown, but is associated with myxoid degeneration.
Mitral valve prolapse is associated with two syndromes:
- Marfan syndrome
- Ehlers-Danlos syndrome
Mitral valve prolapse presents with an incidental mid-systolic click followed by a regurgitation murmur that is usually asymptomatic.
Squatting increases the click and murmur volume of mitral valve prolapse due to increased systemic resistance and slows left ventricular emptying.
Complications of mitral valve prolapse include:
- Infectious endocarditis
- Arrhythmia
- Severe mitral valve regurgitation
Treatment of aortic regurgitation is valve replacement.
 Mitral Valve Prolapse. Heart mitral prolapse Patrick J. Lynch, medical illustrator - Patrick J. Lynch, medical illustrator. Not altered. CC BY 2.5
Mitral Valve Prolapse. Heart mitral prolapse Patrick J. Lynch, medical illustrator - Patrick J. Lynch, medical illustrator. Not altered. CC BY 2.5




Mitral Regurgitation
Mitral regurgitation occurs when blood flows from the left ventricle into the left atrium during systole and is mainly caused by mitral valve prolapse.
Causes of mitral regurgitation include:
- Acute rheumatic heart disease
- Papillary muscle rupture following a myocardial infarction
- Left ventricle dilatation
- Infective endocarditis
Clinical features of mitral regurgitation include:
- A holosystolic blowing murmur that becomes louder with squatting due to higher systemic resistance
- Decreased left ventricular emptying
- Greater return to the left atrium on expiration
Mitral regurgitation may cause volume overload as well as left-sided cardiac failure.
 Mitral regurgitation. echocardiogram of severe mitral regurgitation J. Heuser JHeuser. Not altered. CC BY-SA 3.0
Mitral regurgitation. echocardiogram of severe mitral regurgitation J. Heuser JHeuser. Not altered. CC BY-SA 3.0




Mitral Stenosis
The narrowing of the mitral valve orifice is known as mitral stenosis.
Mitral stenosis is associated with persistent rheumatic valve disease.
Clinical findings of mitral stenosis include:
- An opening snap followed by a diastolic rumbling
- Volume overload that causes the left atrium to enlarge
- Pulmonary congestion with edema and alveolar hemorrhage
- Pulmonary hypertension
- Possibly right-sided heart failure
Mitral stenosis may cause atrial fibrillation with associated risk for mural thrombi.
 Mitral Stenosis. Illustration of mitral valvuloplasty Blausen Medical Communications, Inc. Not altered. CC BY 2.0
Mitral Stenosis. Illustration of mitral valvuloplasty Blausen Medical Communications, Inc. Not altered. CC BY 2.0