Vasculitis
Vasculitis is inflammation of the blood vessel wall.
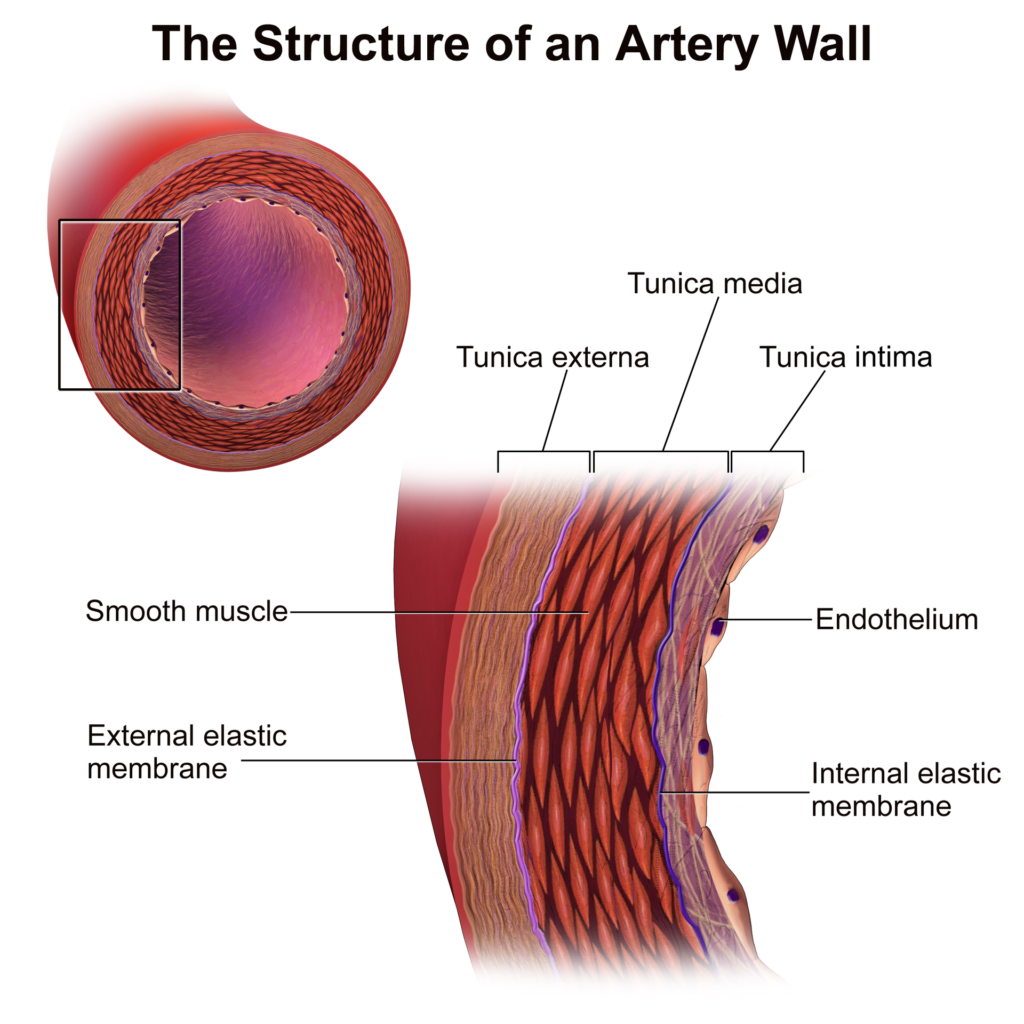
The arterial wall is made of three layers which include:
- Tunica intima (endothelial intima)
- Tunica media (smooth muscle)
- Adventitia (connective tissue adventitia)
Most instances of vasculitis have an unknown etiology.
Most instances of vasculitis are not contagious.
Clinical features associated with vasculitis include:
- Fever
- Fatigue
- Muscle pain (myalgia)
- Weight loss
Some vasculitides may cause organ ischemia due to thrombosis or luminal constriction of inflammatory vessels.
Vasculitis is classified into:
- Large vessel vasculitis
- Medium vessel vasculitis
- Small vessel vasculitis
The aorta and its major branches are affected by large vessel vasculitis.
Muscular arteries that supply organs are involved in medium vessel vasculitis.
Arterioles, capillaries, and venules are all involved in small vessel vasculitis.
 Vasculitis. Severe vasculitis of the major vessels, displayed on FDG-PET/CT - Not altered. CC BY-SA 3.0
Vasculitis. Severe vasculitis of the major vessels, displayed on FDG-PET/CT - Not altered. CC BY-SA 3.0





 Arteritis 1")

Large Vessel Vasculitis
Temporal (Giant Cell) Arteritis
Temporal (giant cell) arteritis is a granulomatous vasculitis that typically affects branches of the carotid artery (i.e. the temporal artery).
Temporal (giant cell) arteritis affects females more than males.
Temporal (giant cell) arteritis usually affects individuals that are considered elderly.
Symptoms include of temporal (giant cell) arteritis classically include:
- Headache
- Jaw claudication
- Vision problems (ophthalmic artery involvement)
- Frequent flu-like symptoms
- Joint pain
- Muscle pain
Lab findings of temporal (giant cell) arteritis include:
- Elevated erythrocyte sedimentation rate (ESR)
Temporal (giant cell) arteritis lesions are segmental, and long segments of vessels must be biopsied for the diagnosis.
Temporal (giant cell) arteritis is not excluded by a negative biopsy result.
Histologic assessment of the temporal artery of a patient with temporal (giant cell) arteritis classically shows an inflammatory artery wall with giant cells and intimal fibrosis.
Temporal (giant cell) arteritis is treated with corticosteroids.
Blindness is a risk factor of temporal (giant cell) arteritis, especially if it is not treated.
 Arteritis") Temporal (Giant Cell) Arteritis. Histopathology of giant cell vasculitis in a cerebral artery. Elastica-stain. Marvin 101 - Not altered. CC BY-SA 3.0
Temporal (Giant Cell) Arteritis. Histopathology of giant cell vasculitis in a cerebral artery. Elastica-stain. Marvin 101 - Not altered. CC BY-SA 3.0
Takayasu Arteritis
Aortic arch branch points are typically affected by granulomatous vasculitis in Takayasu arteritis.
Takayasu arteritis is also known as pulseless disease.
Takayasu arteritis is a condition that typically affects young Asian female adults.
Symptoms of Takayasu arteritis includes:
- Visual issues
- Neurological symptoms
- Weak or nonexistent pulse in the upper extremities
Lab findings of Takayasu arteritis include:
- Elevated erythrocyte sedimentation rate (ESR)
Takayasu arteritis is treated by corticosteroids.
 Takayasu Arteritis. Axial T1-weighted post-gadolinium MRI in a patient with Takayasu arteritis showing thickened, enhancing aortic wall, consistent with large vessel vasculitis Dr Laughlin Dawes. Not altered. CC BY-SA 3.0
Takayasu Arteritis. Axial T1-weighted post-gadolinium MRI in a patient with Takayasu arteritis showing thickened, enhancing aortic wall, consistent with large vessel vasculitis Dr Laughlin Dawes. Not altered. CC BY-SA 3.0


Medium Vessel Vasculitis
Polyarteritis Nodosa
Polyarteritis nodosa is a multisystemic disorder characterized by widespread inflammation, small and medium vessel damage.
Organs commonly involved by polyarteritis nodosa include:
- Skeletal muscles
- Nervous systems
- Gastrointestinal system
- Kidneys
- Cardiovascular system
The lungs are typically spared in polyarteritis nodosa.
Symptoms of polyarteritis nodosa typically include:
- Hypertension due to involvement of the renal arteries
- Stomach pain with melena due to involvement of the mesenteric vessels
- Neurologic abnormalities
- Skin lesions
Polyarteritis nodosa is associated with serum HBsAg.
Histopathology of polyarteritis nodosa shows transmural inflammation and fibrinoid necrosis early on.
Fibrosis may present later on as a ‘string-of-pearls’ appearance on imaging.
Polyarteritis nodosa is treated with corticosteroids and cyclophosphamide.
Polyarteritis nodosa is lethal if not treated.
 Polyarteritis Nodosa. - A. Kussmaul, R. Maier: Not altered Public Domain
Polyarteritis Nodosa. - A. Kussmaul, R. Maier: Not altered Public Domain




Kawasaki Disease
Kawasaki disease causes vascular inflammation of medium sized vessels.
Kawasaki disease typically affects children of Asian descent.
Symptoms of Kawasaki disease include:
- Fever
- Conjunctivitis
- Palmar rash
- Rash on soles
- Lymphadenopathy
In Kawasaki disease the coronary artery is usually involved, and increases the risk of myocardial infarction with thrombosis and aneurysm rupture.
Kawasaki disease is treated by aspirin and IVIg.
Most children with Kawasaki disease completely recover.
 Kawasaki Disease. Kawasaki disease: Strawberry tongue and bright red, swollen lips with vertical cracking and bleeding. Kawasaki_symptoms.jpg: Dong Soo Kim derivative work: Not altered. CC BY 2.0
Kawasaki Disease. Kawasaki disease: Strawberry tongue and bright red, swollen lips with vertical cracking and bleeding. Kawasaki_symptoms.jpg: Dong Soo Kim derivative work: Not altered. CC BY 2.0




Buerger’s Disease
Buerger’s disease is a type of vasculitis that causes necrosis of the fingers and toes.
Symptoms of Buerger’s disease include:
- Auto-amputation of the digits (fingers and toes)
- Gangrene of the digits
- Ulceration of the digits
Raynaud phenomenon is usually present in Buerger’s disease.
Buerger’s disease is highly related to heavy smoking.
There is no cure for Buerger’s disease.
Buerger’s disease progression is halted by smoking cessation.
 Buerger Disease. Morbus Buerger, CT angiogram Milorad Dimic MD - Not altered. GFDL
Buerger Disease. Morbus Buerger, CT angiogram Milorad Dimic MD - Not altered. GFDL


Small Vessel Vasculitis
Wegener Granulomatosis
Wegener granulomatosis is a necrotizing granulomatous vasculitis that affects the kidneys, lungs, and nasopharynx.
Wegener granulomatosis is a middle-aged man with:
- Sinusitis
- Nasopharyngeal ulcer
- Hemoptysis
- Bilateral nodular lung infiltrates
- Hematuria
- Glomerulonephritis
Wegener granulomatosis disease activity is correlated with serum c-ANCA concentrations.
The histology of vessels affected by Wegener granulomatosis show large necrotizing granulomas and nearby necrotizing vasculitis.
Wegener granulomatosis is treated with cyclophosphamide and steroids.
Relapses are common for Wegener granulomatosis.
 Wegener Granulomatosis. Photo showing the sclerokeratitis associated with GPA Jonathan Trobe, M.D. - Not altered. CC BY 3.0
Wegener Granulomatosis. Photo showing the sclerokeratitis associated with GPA Jonathan Trobe, M.D. - Not altered. CC BY 3.0








Microscopic Polyangiitis (MPA)
Microscopic polyangiitis (MPA) is a necrotizing vasculitis that affects many organs, including the kidney and lung.
Although there is no nasopharyngeal involvement and no granulomas in microscopic polyangiitis (MPA), the presentation is similar to Wegener granulomatosis.
Microscopic polyangiitis (MPA) disease activity is correlated with serum levels of p-ANCA.
Microscopic polyangiitis (MPA) is treated by corticosteroids and cyclophosphamide.
Microscopic polyangiitis (MPA) is prone to relapses.
 Microscopic Polyangiitis. Ultra-wide-field fundus photographs of a patient with microscopic polyangiitis showing relatively normal appearing retinas in both eyes. Ultra-Wide-Field Fluorescein Angiography in Microscopic Polyangiitis. Case Reports in Ophthalmological Medicine. Not altered. CC.
Microscopic Polyangiitis. Ultra-wide-field fundus photographs of a patient with microscopic polyangiitis showing relatively normal appearing retinas in both eyes. Ultra-Wide-Field Fluorescein Angiography in Microscopic Polyangiitis. Case Reports in Ophthalmological Medicine. Not altered. CC.

Churg-Strauss Syndrome
In Churg-Strauss syndrome multiple organs are affected by a necrotizing, granulomatous inflammation with eosinophils, particularly the heart and lungs.
Churg-Strauss syndrome is also associated with peripheral eosinophilia and asthma.
Churg-Strauss syndrome disease activity is correlated with serum p-ANCA concentrations.
 Churg-Strauss Syndrome. High magnification micrograph of eosinophilic vasculitis consistent with Churg-Strauss syndrome, abbreviated CSS. H&E stain. CSS is characterized by: Granulomas. Asthma. Fever. Eosinophilia. Related images High mag. Very high mag. Nephron - Not altered. CC BY-SA 3.
Churg-Strauss Syndrome. High magnification micrograph of eosinophilic vasculitis consistent with Churg-Strauss syndrome, abbreviated CSS. H&E stain. CSS is characterized by: Granulomas. Asthma. Fever. Eosinophilia. Related images High mag. Very high mag. Nephron - Not altered. CC BY-SA 3.

Henoch-Schönlein Purpura
Henoch-Schönlein purpura (HSP) is a vasculitis caused by the deposition of the lgA immune complex.
Henoch-Schönlein purpura (HSP) is the most common vasculitis in the pediatric population.
Symptoms of Henoch-Schönlein purpura (HSP) include:
- Hematuria
- GI pain
- Bleeding
- A characteristic rash described as palpable purpura on the buttocks and legs
Henoch-Schönlein purpura (HSP) happens frequently after an upper respiratory tract infection.
Henoch-Schönlein purpura (HSP) illness is self-limited but may return.
If severe Henoch-Schönlein purpura (HSP) is treated with corticosteroids.
 Henoch-Schonlein Purpura. Microphotograph of a histological section of human skin prepared for direct immunofluorescence using an anti-IgA antibody, the skin is a biopsy of a patient with Henoch–Schönlein purpura. IgA deposits are found in the walls of small superficial capillaries (yellow arrows). The pale wavy green area on top is the epidermis, the bottom fibrous area is the dermis. Emmanuelm at en.wikipedia. Not altered. CC BY 3.0
Henoch-Schonlein Purpura. Microphotograph of a histological section of human skin prepared for direct immunofluorescence using an anti-IgA antibody, the skin is a biopsy of a patient with Henoch–Schönlein purpura. IgA deposits are found in the walls of small superficial capillaries (yellow arrows). The pale wavy green area on top is the epidermis, the bottom fibrous area is the dermis. Emmanuelm at en.wikipedia. Not altered. CC BY 3.0





