This is the dysfunction or the rejection of the graft within days after the transplant. This is the result of donor-specific antibodies. Histopathology reveals the endothelial injury mediated by the antibodies. It is less severe than hyperacute antibody-mediated rejections.
What are Acute Antibody-Mediated Rejections?
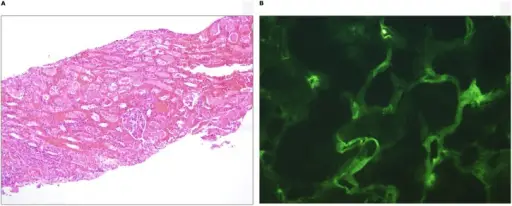
A) A 4-year-old child who had good allograft function initially and then developed acute antibody-mediated rejection 2 weeks after deceased donor kidney transplantation. Renal biopsy reveals marked acute tubular necrosis and interstitial hemorrhage. There is evidence of glomerulitis and tubulitis (H&E, 40×). B) Immunofluorescence in this patient reveals diffuse C4d staining of the peritubular capillaries, supporting the diagnosis of acute antibody-mediated rejection.Issues in solid-organ transplantation in children: translational research from bench to bedside.
Lipshultz SE, Chandar JJ, Rusconi PG, Fornoni A, Abitbol CL, Burke GW, Zilleruelo GE, Pham SM, Perez EE, Karnik R, Hunter JA, Dauphin DD, Wilkinson JD - Clinics (São Paulo, Brazil) (2014). Not Altered. CC.
Post navigation
Previous Post
 What is Hyperacute Rejection?
What is Hyperacute Rejection?