Mammosomatotroph adenomas are both GH and prolactin secreting tumors.
Associated syndromes include symptoms and syndromes of prolactin and growth hormone excess:
- Galactorrhea
- Infertility
- Sexual dysfunction
- Gigantism
- Acromegaly
What is the Pathology of Mammosomatotroph Adenomas?
The pathology of mammosomatotroph adenomas is:
-Etiology: The cause of mammosomatotroph adenomas is consolidation of molecular genetic changes and hormonal stimulation acting as a promoter.
-Genes involved: gene PRKAR1A, Menin (11q13).
-Pathogenesis: The sequence of events that lead to mammosomatotroph adenomas. Arises from growth of pituitary lactotrophs and somatotroph cell. The mutation and activation of Gsα result in the generation of cyclic adenosine monophosphate (cAMP), a potent mitogenic stimulus for variety of endocrine cell types, hence endorsing hormone synthesis and secretion and cellular proliferation.
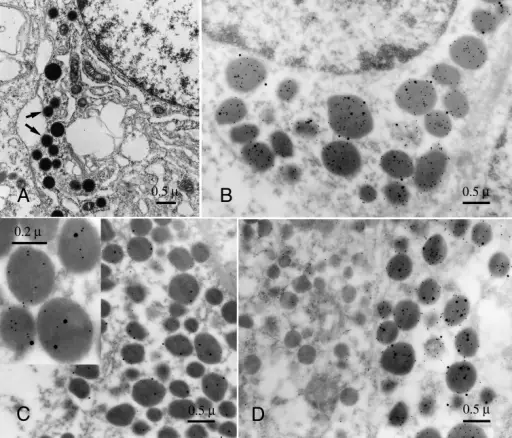
-Morphology: The morphology associated with mammosomatotroph adenomas shows quite large adenoma.
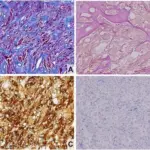
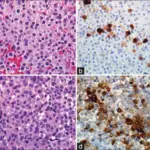
-Histology: The histology associated with mammosomatotroph adenomas shows acidophilic on H & E staining.
How does Mammosomatotroph Adenomas Present?
Patients with mammosomatotroph adenomas typically more women than male present at age range of 20 to 45 years. The symptoms, features, and clinical findings associated with mammosomatotroph adenomas include acromegaly and hyperprolactinemia.
How is Mammosomatotroph Adenomas Diagnosed?
Mammosomatotroph adenomas is diagnosed through laboratory studies complex IHC study. Imaging studies such as high-resolution CT scan and/or MRI suggest an incidental lesion.
How is Mammosomatotroph Adenomas Treated?
Mammosomatotroph adenomas is treated dopamine antagonist, GH receptor antagonist and somatostatin receptor ligands, Surgical interventions.
What is the Prognosis of Mammosomatotroph Adenomas?
The prognosis of mammosomatotroph adenomas is poor, tend to be more aggressive than pure adenomas.