Pediatric cardiovascular anomalies are congenital heart defects that mean that a child was born with a problem in the structure of his or her heart.
What is the Pathology of Pediatric Cardiovascular Anomalies?
The pathology of pediatric cardiovascular anomalies is:
-Etiology: The cause of pediatric cardiovascular anomalies is genetics, certain medical conditions, some medications, and environmental or lifestyle factors, such as smoking.
-Genes involved: TBX2, TBX20, TBX3, TBX5, etc.
-Pathogenesis: The sequence of events that lead to pediatric cardiovascular anomalies is abnormal connections that allow blood to flow where it normally wouldn’t, for example, holes in the walls between heart chambers. Heart valve problems include stenosis- valves that are narrowed and don’t open completely or regurgitation- valves that don’t close completely.
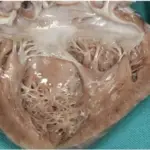
-Morphology: The morphology associated with pediatric cardiovascular anomalies shows a combination of 4 defects: a hole in the wall between the heart’s ventricles, a narrowed passage between the right ventricle and pulmonary artery, a shift in the connection of the aorta to the heart, and thickened muscle in the right ventricle.
How do Pediatric Cardiovascular Anomalies Present?
Patients with pediatric cardiovascular anomalies typically are either males or females present at the age range of infants. The symptoms, features, and clinical findings associated with pediatric cardiovascular anomalies include pale gray or blue skin color (cyanosis), rapid breathing, swelling in the legs, belly, or areas around the eyes, and shortness of breath during feedings, leading to poor weight gain. In older children, symptoms may include easily becoming short of breath during exercise or activity, easily tiring during exercise or activity, fainting during exercise or activity, and swelling in the hands, ankles, or feet.
How are Pediatric Cardiovascular Anomalies Diagnosed?
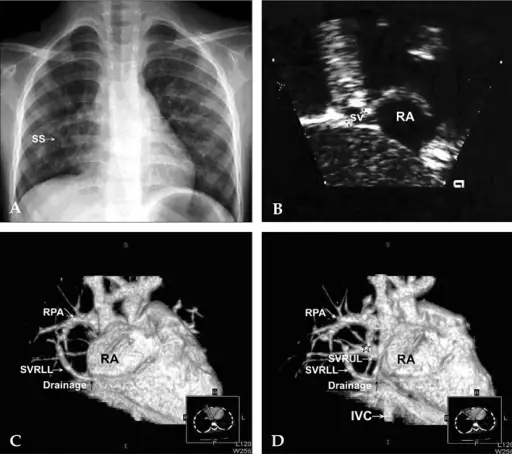
Pediatric cardiovascular anomalies are diagnosed with pulse oximetry, electrocardiogram, echocardiogram, chest X-ray, cardiac catheterization, and heart magnetic resonance imaging (MRI).
How are Pediatric Cardiovascular Anomalies Treated?
Pediatric cardiovascular anomalies are treated with medications that include blood pressure drugs (angiotensin-converting enzyme (ACE) inhibitors, angiotensin II receptor blockers (ARBs), and beta-blockers), diuretics, and heart rhythm drugs (antiarrhythmics). Surgery and heart procedures include fetal cardiac intervention, cardiac catheterization, heart surgery, and heart transplant.
What is the Prognosis of Pediatric Cardiovascular Anomalies?
The prognosis of pediatric cardiovascular anomalies is good. Living with a congenital heart defect can make some children feel stressed or anxious and talking to a therapist or counselor may help them learn new ways to manage stress and anxiety.