Peripheral T-Cell Neoplasms are a group of aggressive lymphomas that develop from mature-stage white blood cells, T cells and NK cells.
Examples of Peripheral T-Cell Neoplasms include:
- T-cell prolymphocytic leukemia
- Large granular lymphocytic leukemia
- Mycosis fungoides
- Sézary syndrome
- Anaplastic large-cell lymphoma
- Angioimmunoblastic T-cell lymphoma
- Enteropathy-associated T-cell lymphoma
- Panniculitis-like T-cell lymphoma
- Hepatosplenic γδT-cell lymphoma
- Adult T-cell leukemia/lymphoma
- Peripheral T-cell lymphoma, unspecified
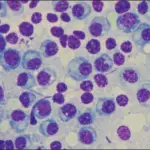
 Peripheral T-Cell Neoplasms_Histology. Montage of pathology images for several different T- and NK- cell lymphomas in children and adolescents. (a) T-LBL showing diffuse infiltration of T-lymphoblasts with fine nuclear chromatin and scarce cytoplasm. Blasts have inconspicuous nucleoli and irregular nuclear contours. × 200 magnification, hematoxylin and eosin (H&E) stain. (b) ALCL, ALK+, showing large neoplastic cells with marked pleomorphism and abundant cytoplasm. Characteristic horseshoe-shaped cells are seen. Cells stained strongly with CD30 and ALK antibodies demonstrate a mature T-cell immunophenotype. × 400 magnification, H&E. (c) PTCL, NOS with predominantly large cell morphology. Neoplastic cells are large with abundant cytoplasm and variably prominent nucleoli. Immunophenotyping reveals a mature T-cell phenotype, but cells lack expression of CD30 or ALK. × 400 magnification, H&E. (d) Hepatosplenic γ/δ T-cell lymphoma. Small-to-intermediate neoplastic cells have infiltrated liver sinusoids. These cells show round nuclear contours, clumped chromatin without prominent nucleoli, and abundant clear cytoplasm. × 100 magnification, H&E. (e) SPTCL demonstrating invasion of malignant cells into fat. Small-to-intermediate size neoplastic cells with moderate cytologic atypia and irregular nuclear contours surround fat lobules. × 400 magnification, H&E. (f) Primary cutaneous γ/δ T-cell lymphoma that presented with skin nodules and plaques with extensive dermal involvement and extension into panniculitic fat. Medium-to-large neoplastic cells have occasional prominent nucleoli. Neoplastic cells lacked CD4 and CD8 expression and were EBV negative. × 200 magnification, H&E. (g) T-cell post-transplant lymphoproliferative disorder in a patient with liver transplant 2 years prior. Clonal T cells have invaded the intestine and are EBV positive. × 400 magnification, H&E. (h) Extranodal T/NK-cell lymphoma of the nasal cavity showing angiocentric pattern with vascular invasion. Neoplastic cells are small-to-intermediate in size with abundant cytoplasm. Irregular nuclei show clumped hyperchromatic chromatin. Cells are CD8 and EBV positive. × 200 magnification, H&E. (i) AITL with diffuse nodal effacement and prominent arborizing vessels. Neoplastic cells are intermediate size and show variable clear cytoplasm. × 200 magnification, H&E. Pediatric T- and NK-cell lymphomas: new biologic insights and treatment strategies. El-Mallawany NK, Frazer JK, Van Vlierberghe P, Ferrando AA, Perkins S, Lim M, Chu Y, Cairo MS - Blood cancer journal (2012). Not altered. CC.
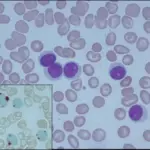
Peripheral T-Cell Neoplasms_Histology. Montage of pathology images for several different T- and NK- cell lymphomas in children and adolescents. (a) T-LBL showing diffuse infiltration of T-lymphoblasts with fine nuclear chromatin and scarce cytoplasm. Blasts have inconspicuous nucleoli and irregular nuclear contours. × 200 magnification, hematoxylin and eosin (H&E) stain. (b) ALCL, ALK+, showing large neoplastic cells with marked pleomorphism and abundant cytoplasm. Characteristic horseshoe-shaped cells are seen. Cells stained strongly with CD30 and ALK antibodies demonstrate a mature T-cell immunophenotype. × 400 magnification, H&E. (c) PTCL, NOS with predominantly large cell morphology. Neoplastic cells are large with abundant cytoplasm and variably prominent nucleoli. Immunophenotyping reveals a mature T-cell phenotype, but cells lack expression of CD30 or ALK. × 400 magnification, H&E. (d) Hepatosplenic γ/δ T-cell lymphoma. Small-to-intermediate neoplastic cells have infiltrated liver sinusoids. These cells show round nuclear contours, clumped chromatin without prominent nucleoli, and abundant clear cytoplasm. × 100 magnification, H&E. (e) SPTCL demonstrating invasion of malignant cells into fat. Small-to-intermediate size neoplastic cells with moderate cytologic atypia and irregular nuclear contours surround fat lobules. × 400 magnification, H&E. (f) Primary cutaneous γ/δ T-cell lymphoma that presented with skin nodules and plaques with extensive dermal involvement and extension into panniculitic fat. Medium-to-large neoplastic cells have occasional prominent nucleoli. Neoplastic cells lacked CD4 and CD8 expression and were EBV negative. × 200 magnification, H&E. (g) T-cell post-transplant lymphoproliferative disorder in a patient with liver transplant 2 years prior. Clonal T cells have invaded the intestine and are EBV positive. × 400 magnification, H&E. (h) Extranodal T/NK-cell lymphoma of the nasal cavity showing angiocentric pattern with vascular invasion. Neoplastic cells are small-to-intermediate in size with abundant cytoplasm. Irregular nuclei show clumped hyperchromatic chromatin. Cells are CD8 and EBV positive. × 200 magnification, H&E. (i) AITL with diffuse nodal effacement and prominent arborizing vessels. Neoplastic cells are intermediate size and show variable clear cytoplasm. × 200 magnification, H&E. Pediatric T- and NK-cell lymphomas: new biologic insights and treatment strategies. El-Mallawany NK, Frazer JK, Van Vlierberghe P, Ferrando AA, Perkins S, Lim M, Chu Y, Cairo MS - Blood cancer journal (2012). Not altered. CC.