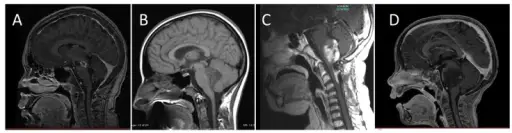
Diffuse intrinsic pontine glioma (DIPG) is an infiltrative, expansile non-enhancing T2 hyper-intense lesion that involves the brainstem. Findings are nonspecific, but a diffuse midline glioma should be a primary consideration. Note that an inflammatory process cannot be absolutely excluded.
What is the Pathology of Diffuse Intrinsic Pontine Glioma?
The pathology of diffuse intrinsic pontine glioma is:
-Etiology: The cause of diffuse intrinsic pontine glioma is thought to be from an oligodendrocyte precursor cell or, olig2-/nestin- neural precursor like cells.
-Genes involved: H3 K27M.
-Pathogenesis: The sequence of events that lead to diffuse intrinsic pontine glioma is malignant cell proliferation and potential mass effect on the brainstem.
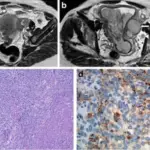
-Histology: The histology associated with diffuse intrinsic pontine glioma classically shows pseudo-palisading necrosis and microvascular proliferation.
-Stains:
- Olig2 or GFAP
- Ki-67
- p53
- H3K27M
- IDH-1
How does Diffuse Intrinsic Pontine Glioma Present?
Patients with diffuse intrinsic pontine glioma typically present with neurologic symptoms involving brainstem cranial nerves.
Symptoms may include:
- Double vision
- Facial weakness
- Difficulty chewing
- Difficulty swallowing
How is Diffuse Intrinsic Pontine Glioma Diagnosed?
Diffuse intrinsic pontine glioma is diagnosed typically by radiology (MRI).
How is Diffuse Intrinsic Pontine Glioma Treated?
Diffuse intrinsic pontine glioma is treated with radiation therapy or chemotherapy. Radiation therapy is not curative, but is meant to be temporary procedures. Chemotherapy is aimed at improving survival.
What is the Prognosis of Diffuse Intrinsic Pontine Glioma?
The prognosis of diffuse intrinsic pontine glioma is poor. The 5 year survival rate is less than 1%. These tumors are not classified by grade. Note that taking a biopsy or surgical resection of the lesion is typically not safe due to the location of the tumor. If the tumor is amenable to biopsy, they are typically grade III or grade IV.