Duplication of the gallbladder is a rare congenital malformation that occurs in about one in 4000 births.
What is the Pathology of Duplication of the Gallbladder?
The pathology of duplication of the gallbladder is:
-Etiology: The cause of duplication of the gallbladder is associated with an increased risk of complications after laparoscopic cholecystectomy. It can’t be accurately assessed, since the only cases which have been identified are those that became symptomatic or were encountered as incidental findings during surgery, imaging studies, or at autopsy.
-Genes involved: Unknown.
-Pathogenesis: The sequence of events that lead to duplication of the gallbladder is that it occurs when either the cystic primordium splits during the fifth to sixth weeks of embryogenesis to give a duplicate gallbladder or when there’s extra budding of the biliary primordium to give rise to an accessory gallbladder.
-Morphology: The morphology associated with duplication of the gallbladder shows two chambers with a single cystic duct that communicate through a common ostium and there are two cystic arteries as well.
How does the Duplication of the Gallbladder Present?
Patients with duplication of the gallbladder typically are either male or female present at the age range of older than 65 years. The symptoms, features, and clinical findings associated with duplication of the gallbladder include acute or chronic cholecystitis, cholelithiasis, empyema, torsion, cholecystocolic fistula, and carcinoma.
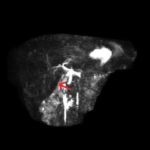
How is Duplication of the Gallbladder Diagnosed?
Duplication of the gallbladder is diagnosed by preoperative imaging.
How is Duplication of the Gallbladder Treated?
Duplication of the gallbladder is treated by laparoscopic cholecystectomy with intraoperative cholangiography in the symptomatic gallbladder and the removal of an asymptomatic double gallbladder remains controversial.
What is the Prognosis of Duplication of the Gallbladder?
The prognosis of duplication of the gallbladder is good and the simultaneous removal of both gallbladders at surgery is recommended to avoid cholecystitis and biliary colic in the remaining organ.