Primary hyperaldosteronism is a medical condition wherein too much aldosterone. This can lead to lowered levels of potassium in the blood (hypokalemia) and increased hydrogen ion excretion (alkalosis).
What is the Pathology of Hyperaldosteronism?
The pathology of hyperaldosteronism is:
-Etiology: The cause of hyperaldosteronism are adrenal hyperplasia and adrenal adenoma (Conn’s syndrome) for primary hyperaldosteronism and accessory renal veins, fibromuscular dysplasia, reninoma, renal tubular acidosis, nutcracker syndrome, ectopic tumors, massive ascites, left ventricular failure, and cor pulmonale for secondary hyperaldosteronism.
-Genes involved: 7p22.
-Pathogenesis: The sequence of events that lead to hyperaldosteronism is an adrenal adenoma, termed Conn’s syndrome, bilateral idiopathic adrenal hyperplasia, congenital adrenal hyperplasia, and adrenal carcinoma that is extremely rare. Secondary hyperaldosteronism (also hyperreninism, or hyperreninemic hyperaldosteronism) is due to overactivity of the renin–angiotensin–aldosterone system (RAAS).
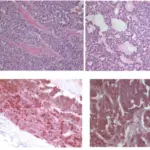
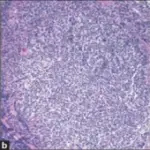
-Morphology: The morphology associated with hyperaldosteronism shows adenomas that are small, unilateral, solitary, and golden-yellow.
-Histology: The histology associated with hyperaldosteronism shows thickened glomerulosa layer with tongue-like projections into fasciculata, spironolactone bodies in patients treated with spironolactone, and variable micronodules of clear cells.
How does Hyperaldosteronism Present?
Patients with hyperaldosteronism typically are either male or female present at the age range of 30 to 50 years old. The symptoms, features, and clinical findings associated with hyperaldosteronism include weakness, paresthesias, visual disturbances, tetany, and hypertension.
How is Hyperaldosteronism Diagnosed?
Hyperaldosteronism is diagnosed with a blood test to check for the aldosterone-to-renin ratio.
How is Hyperaldosteronism Treated?
Hyperaldosteronism is treated with surgery for adrenal adenoma. Secondary hyperaldosteronism may be treated with cox-2 inhibitors which cause water retention, sodium retention, and potassium retention as well as raising blood pressure.
What is the Prognosis of Hyperaldosteronism?
The prognosis of hyperaldosteronism is fair with proper treatment.