Megaloblastic anemia is the reduction of hematocrit and hemoglobin levels as a result of deficiencies of vital nutrients necessary for red cell formation. Megaloblastic anemia may be due to pernicious anemia, vitamin B12 deficiency. It may also be due to vitamin B9 deficiency.
What is the Pathology of Megaloblastic Anemia?
The pathology of megaloblastic anemia is:
-Etiology: The cause of megaloblastic anaemia is Pernicious anaemia, bacterial overgrowth in the intestine, folic acid deficiency, and certain drugs.
-Genes involved: None.
-Pathogenesis: The sequence of events that lead to megaloblastic anemia may be due to deficiency of vitamin B12 causes pernicious anemia, while deficiency of folic acid leads to folate deficiency anemia (featured by defective DNA synthesis), and iron deficiency anemias characterized by impaired heme production.
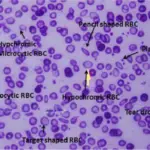
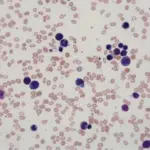
-Morphology: The morphology associated with megaloblastic anemia shows red cells are macrocytic and oval.
-Histology: The histology associated with megaloblastic anemia shows a six-lobed hyper nucleus segmented neutrophil.
How does Megaloblastic Anemia Present?
Patients with megaloblastic anemia are typically higher in females than males present at the age range of 40 years. The symptoms, features, and clinical findings associated with megaloblastic anemia include abdominal discomfort, hyperpigmentation, lethargy, fatigue, faintness, pallor, weight loss, abnormal gait, loss of balance, and headaches.
How is Megaloblastic Anemia Diagnosed?
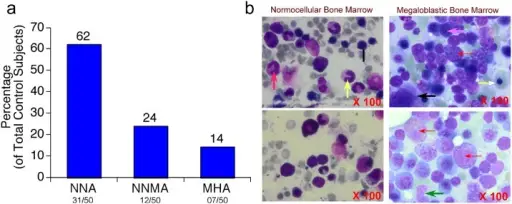
Megaloblastic anemia is diagnosed through the clinical presentation, laboratory studies- red blood cell (RBC) indices, complete blood count, peripheral blood smear reticulocyte, count, Iron and ferritin level, serum folate, and bone marrow aspiration.
How is Megaloblastic Anemia Treated?
Megaloblastic anemia is treated through medical care such as cobalamin therapy, folate therapy, management of other linked conditions. Dietary measures and consultations may be helpful.
What is the Prognosis of Megaloblastic Anemia?
The prognosis of megaloblastic anemia is good when the etiology is identified and managed appropriately.