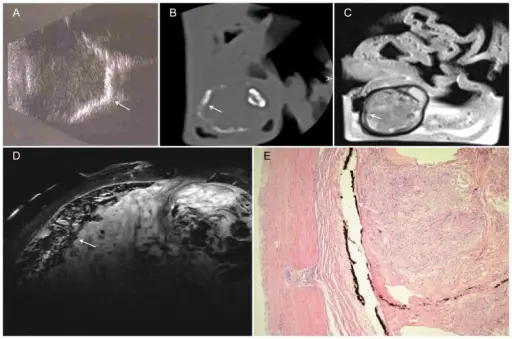
Premature retinopathy with phthisis and calcification of ocular wall (arrow).A – Sonography: Hyperreflective line corresponding to ossification process of bulbar wall. B – CT reconstructed in the bone window: corresponding plane to the MR image; the gross calcifications appear as linear hyperdensities. C – T2w image at 1.5 T: Bulbar wall with very low signal intensity; the vitreous body is of inhomogeneous low signal intensity, and ultrastructures cannot be identified with certainty. D – Sagittal T2w image: Thickened retina with very low signal intensity as a sign of calcification; intraocular scar tissue is characterized by inhomogeneous MR signal intensity. E – H&E stain, 4× magnification: Histologically, the intraocular space is filled with fibromatous scar tissue, and there is ossification of the bulbar wall originating in the pigment epithelium. Experimental differentiation of intraocular masses using ultrahigh-field magnetic resonance imaging--a case series.
Falke K, Krüger P, Hosten N, Zimpfer A, Guthoff R, Langner S, Stachs O - PloS one (2013). Not Altered. CC.
Retrolental fibroplasia is an abnormal replacement of the sensory retina by fibrous tissue and blood vessels.
What is the Pathology of Retrolental Fibroplasia?
The pathology of retrolental fibroplasia is replacement of retina by fibrous tissue and also blood vessels.
How does Retrolental Fibroplasia Present?
Retrolental fibroplasia presents with birth weight less than 1.5kg, tortuosity of vessels.
How is Retrolental Fibroplasia Diagnosed?
Retrolental fibroplasia is diagnosed by dilated fundus examination with scleral depression.
How is Retrolental Fibroplasia Treated?
Retrolental fibroplasia is treated with oral propranolol, intravitreal injection of bevacizumab, scleral buckling, and vitrectomy.
What is the Prognosis of Retrolental Fibroplasia?
The prognosis of retrolental fibroplasia is poor if not properly managed.

