Cervix
The cervix refers to the uterus neck.
The cervix is comprised of:
- Ectocervix (aka exocervix)
- Endocervix
- Transition zone
Nonkeratinizing squamous epithelium lines the ectocervix.
Columnar cells make up the inner layer lining the endocervix.
The transition zone is the area where the exocervix and endocervix meet.
Human papilloma virus (HPV) is a virus that may infect the cervix and promote cancer.
Human papilloma virus (HPV) is a DNA virus.
Spread of human papilloma virus (HPV) is by physical contact and sex.
Acute inflammation typically eliminates infection, and chronic infection increases the chance of cervical dysplasia (cervical intraepithelial neoplasia, CIN).
High risk human papilloma virus (HPV) types include:
- 16
- 18
- 31
- 33
- 35
Low risk human papilloma virus (HPV) types include:
- 6
- 11
E6 and E7 proteins, which are produced by high-risk human papilloma virus (HPV) types.
E6 enhances the degradation of p53.
E7 enhance the degradation Rb.
Cervical intraepithelial neoplasia (CIN) risk is increased when certain tumor suppressor proteins are lost.
 Cervical Cancer Screening. Negative visual inspection with acetic acid of the cervix Haeok Lee1,2*, Mary Sue Makin3, Jasintha T Mtengezo4,5 and Address Malata6 - Not altered. CC BY 4.0
Cervical Cancer Screening. Negative visual inspection with acetic acid of the cervix Haeok Lee1,2*, Mary Sue Makin3, Jasintha T Mtengezo4,5 and Address Malata6 - Not altered. CC BY 4.0
Cervical Intraepithelial Neoplasia (CIN)
Cervical intraepithelial neoplasia (CIN) is characterized by:
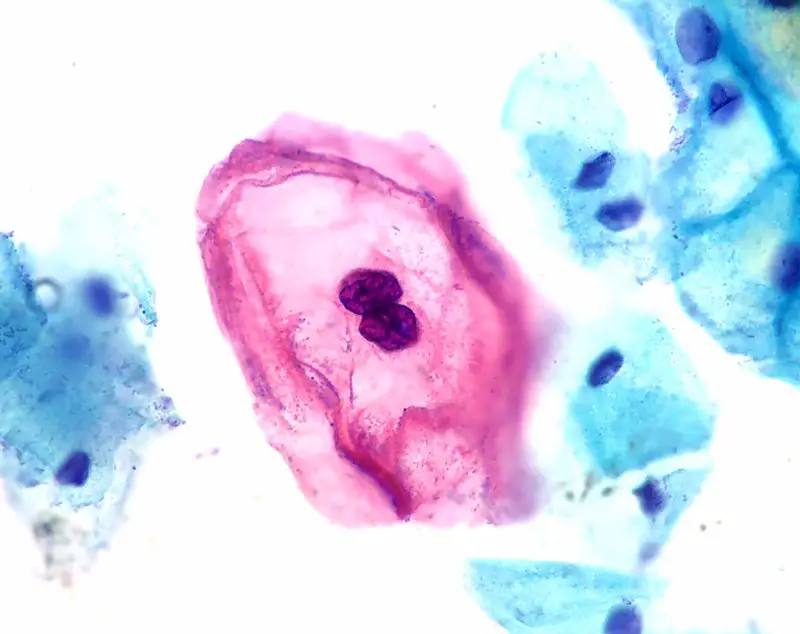
- Koilocytic alteration
- Atypical nuclear morphology
- Abnormal cellular maturation
- Elevated mitotic activity
According to the degree of epithelial involvement by immature dysplastic cells, grades are established as follows:
- Less than the full thickness of the epithelium is involved in CIN I
- About one-third of the epithelium’s thickness is involved in CIN II
- About two-thirds of the epithelium’s thickness is involved in CIN III
The full thickness of the epithelium is affected by carcinoma in situ (CIS).
Cervical intraepithelial neoplasia (CIN) typically develops into invasive squamous cell carcinoma in a stepwise method through CIN I, CIN II, CIN Ill, and CIS.
Progress is not always forward (e.g., CIN I often regresses).
The likelihood that a dysplasia would proceed to cancer and less likelihood that it will revert to normal depends on its grade.
 Cervical Intraepithelial Neoplasia. Positive visual inspection with acetic acid of the cervix for CIN-1 (photo by cervicography) Haeok Lee1,2*, Mary Sue Makin3, Jasintha T Mtengezo4,5 and Address Malata6. Not altered. CC BY 4.0
Cervical Intraepithelial Neoplasia. Positive visual inspection with acetic acid of the cervix for CIN-1 (photo by cervicography) Haeok Lee1,2*, Mary Sue Makin3, Jasintha T Mtengezo4,5 and Address Malata6. Not altered. CC BY 4.0


Cervical Carcinoma
Cervical carcinoma is carcinoma due to the cervical epithelium.
Middle-aged women are the most frequently affected by cervical carcinoma.
Symptoms of cervical carcinoma include:
- Cervical discharge
- Vaginal bleeding
- Postcoital bleeding
Risk factors for cervical carcinoma include:
- High-risk human papilloma virus (HPV) infection is the main risk factor
- Smoking
- Immunodeficiency
Squamous cell carcinoma (SCC) (80% of cases) and adenocarcinoma (15% of cases) are the two most prevalent subtypes of cervical carcinoma.
Both have an association with human papilloma virus (HPV) infection.
Advanced tumors frequently enter the bladder through the front uterine wall and obstruct the ureters.
In advanced cervical cancer, hydronephrosis with postrenal failure is a common cause of mortality.
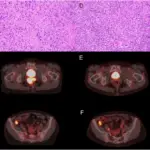
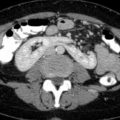
 Cervical Carcinoma with Adnexa.
Cervical Carcinoma with Adnexa.


Cervical Cancer Screening
Detecting dysplasia cervical intraepithelial neoplasia (CIN) before it transforms into cancer is the aim of screening.
On average, cervical intraepithelial neoplasia progression to carcinoma takes 10 to 20 years.
The gold standard for cervical carcinoma screening is a Pap smear.
Starting at age 21, screening is first done once a year.
Using a brush, cells are removed from the transformation zone and examined under a microscope.
Dysplastic cells can be high grade (CIN III) or low grade (CIN I).
Cells with hyperchromatic (black) nuclei and high nuclear to cytoplasmic ratios are characteristics of high-grade dysplasia.
It is to blame for a considerable decrease in cervical cancer morbidity and mortality (cervical carcinoma went from being the most common to one of the least common types of gynecologic carcinoma in the US).
Typically, women with aggressive cervical cancer have not had screenings.
Following a negative Pap smear, a confirmatory colposcopy and biopsy may be necessary.
Adenocarcinoma screening with the Pap smear is not very effective due to insufficient sampling of the transformation zone (false negative screening).
The incidence of adenocarcinoma has not greatly lowered despite Pap smear screening.
Human papilloma virus (HPV) infections can be prevented by vaccination.
Human papilloma virus (HPV) types 6, 11, 16, and 18 are covered by the quadrivalent vaccine.
Condylomas are protected from by antibodies produced against types 6 and 11.
Types 16 and 18 specific antibodies offer protection from cervical intraepithelial neoplasia (CIN) and cancer.
Due to the small number of HPV types that the vaccine can prevent, Pap tests are still required.
 Cervix. A nulliparous woman's ectocervix showing cervical ectropion, visible as the darker red mucosa surrounding the cervical os. Viewed on speculum exam GynaeImages. Not altered. CC BY-SA 4.0
Cervix. A nulliparous woman's ectocervix showing cervical ectropion, visible as the darker red mucosa surrounding the cervical os. Viewed on speculum exam GynaeImages. Not altered. CC BY-SA 4.0