Stomach pathology includes:
- Gastroschisis
- Omphalocele
- Pyloric stenosis
- Acute gastritis
- Chronic gastritis
- Peptic ulcer disease
- Gastric carcinoma
Gastroschisis
Gastroschisis is a congenital malformation of the anterior abdominal wall results in the exposure of abdominal contents.
 Gastroschisis. Gastrochisis in ultrasound: defect is right to midline Mme Mim - Not altered. CC BY-SA 4.0
Gastroschisis. Gastrochisis in ultrasound: defect is right to midline Mme Mim - Not altered. CC BY-SA 4.0


Omphalocele
An omphalocele is a persistent bowel herniation into umbilical cord.
Omphaloceles are caused by the failure of herniated intestines to return to the body cavity during development.
An omphalocele consists of a peritoneum and amnion of the umbilical cord covering the abdominal contents.
 Omphalocele. Diagram showing the process by which the intestine rotates and herniates during normal development. From panel A to B (left-sided views), the midgut loop rotates 90° in a counterclockwise direction, so that its position changes from midsagittal (A) to transverse (B1). The small intestine forms loops (B2) and slides back into the abdomen (B3) during resolution of the hernia. Meanwhile, the cecum moves from the left to the right side, which represents the additional 180° counterclockwise rotation of the intestine (C, central view).[11] Soffers, J.H., Hikspoors, J.P., Mekonen, H.K. et al. Not altered. CC BY 4.0
Omphalocele. Diagram showing the process by which the intestine rotates and herniates during normal development. From panel A to B (left-sided views), the midgut loop rotates 90° in a counterclockwise direction, so that its position changes from midsagittal (A) to transverse (B1). The small intestine forms loops (B2) and slides back into the abdomen (B3) during resolution of the hernia. Meanwhile, the cecum moves from the left to the right side, which represents the additional 180° counterclockwise rotation of the intestine (C, central view).[11] Soffers, J.H., Hikspoors, J.P., Mekonen, H.K. et al. Not altered. CC BY 4.0

Pyloric Stenosis
A pyloric stenosis is due to congenital hypertrophy of pyloric smooth muscle.
Pyloric stenosis is more common in males.
Pyloric stenosis usually presents two weeks after birth.
Symptoms of pyloric stenosis include:
- Projectile nonbilious vomiting
- Visible peristalsis
- Olive-like mass in the abdomen
Pyloric stenosis is treated by myotomy.
Electrolytes may be necessary to replace what was lost during emesis.
 Pyloric Stenosis. Pyloric stenosis as seen on ultrasound in a 6-week-old[13] Dr Laughlin Dawes - Not altered. CC BY-SA 4.0.
Pyloric Stenosis. Pyloric stenosis as seen on ultrasound in a 6-week-old[13] Dr Laughlin Dawes - Not altered. CC BY-SA 4.0.




Acute Gastritis
Acute gastritis is due to inflammation of the stomach mucosa.
Acidic damage to the stomach mucosa may predispose patients to acute gastritis due to an imbalance between mucosal defenses and the acidic environment.
Gastric mucosal defenses include:
- Mucin layer created by foveolar cells
- Bicarbonate secretion by surface epithelium
- Adequate blood supply (gives nutrients and picks up leaked acid)
Risk factors for acute gastritis include:
- Severe burn (Curling ulcer)
- Hypovolemia results in reduced blood supply
- Non-steroidal anti-inflammatory drugs
- Decreased prostaglandins
- Heavy alcohol consumption
- Chemotherapy
Increased intracranial pressure (Cushing ulcer) causes increased stimulation of the vagus nerve which results in increased acid production.
Multiple (stress) ulcers may be visible in the intensive care unit (ICU) patients who are in shock.
Acid injury causes an ulcer, erosion (loss of superficial epithelium), or superficial inflammation (loss of mucosal layer).
 Acute Gastritis. Updated Sydney System for visual classification of gastritis on histopathology. Carrasco G, Corvalan AH - Carrasco G, Corvalan AH. Not altered. CC BY 3.0
Acute Gastritis. Updated Sydney System for visual classification of gastritis on histopathology. Carrasco G, Corvalan AH - Carrasco G, Corvalan AH. Not altered. CC BY 3.0




Chronic Gastritis
Chronic gastritis is due to inflammation of stomach mucosa.
Chronic gastritis is classified into two types based on underlying etiology:
- Chronic autoimmune gastritis
- Chronic H. pylori gastritis
Chronic Autoimmune Gastritis
Chronic autoimmune gastritis is the autoimmune destruction of gastric parietal cells, which are found in the stomach body and fundus.
Chronic autoimmune gastritis is linked to parietal cell and/or intrinsic factor antibodies.
Clinical features of chronic autoimmune gastritis include:
- Atrophy of mucosa with intestinal metaplasia
- Achlorhydria with antral G-cell hyperplasia and elevated gastrin levels
- Megaloblastic (pernicious) anemia because of lack of intrinsic factor
Patients with chronic autoimmune gastritis have increased risk for gastric adenocarcinoma (intestinal type).
Chronic H. Pylori Gastritis
Chronic H. pylori gastritis is because of H. pylori-induced acute and chronic inflammation.
Chronic gastritis due to H. pylori is the most typical type of gastritis (90 percent).
Mucosal defenses are weakened by H. pylori ureases and proteases as well as inflammation.
The antrum is the most common site of involvement by chronic H. pylori gastritis.
Symptoms of chronic H. pylori gastritis include:
- Vague abdominal pain
- Diarrhea
In chronic H. pylori gastritis, there is increased risk for:
- High risk for ulceration (peptic ulcer disease)
- Gastric adenocarcinoma (intestinal type)
- Mucosal associated lymphoid tissue (MALT) lymphoma
Treatment of chronic H. pylori gastritis involves triple therapy, which includes:
- A proton pump inhibitor (PPI) (e.g. omeprazole)
- Clarithromycin (antibiotic)
- Amoxicillin or metronidazole (antibiotic)
Treatment of chronic H. pylori gastritis usually resolves gastritis and reverses intestinal metaplasia.
The absence of stool antigen and a negative urea breath test both attest to the eradication of H. pylori.
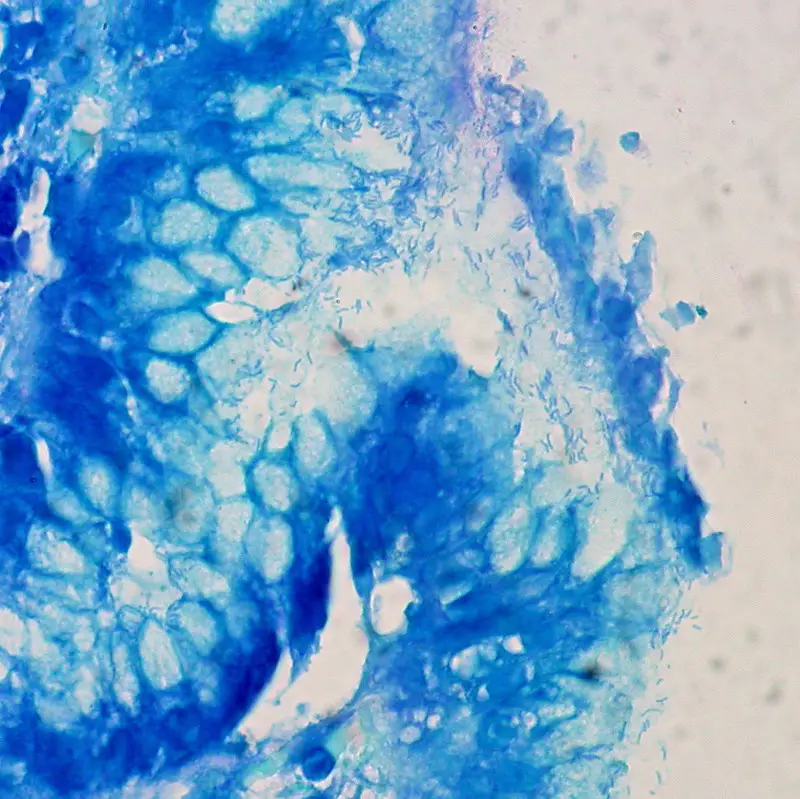
 Antral mucosa. Normal (A): Normal number of antral G cells with typical “hallo” appearances occur in neck area of the pyloric glands (arrows). Non-atrophic chronic gastritis (B): Mononuclear inflammation occupies the whole mucosa giving an impression of gland loss (atrophy). Atrophic gastritis of mild to moderate degree in antrum (C): Inflammation is relative mild but there is a large area of pyloric glands lost and replaced with metaplastic glands (IM) as indicated with arrows. Severe atrophic gastritis in antrum (D): All pyloric glands are gone and the whole mucosa is “intestinalized”. Inflammation is mild, or moderate at most. Also the antral G cells are disappeared along with the loss of the normal pyloric glands. Therefore, the G-17 feedback response in physiological control of acid secretion is impaired. HE and Alcian blue – PAS stains × 300. Chronic gastritis. Sipponen P, Maaroos HI - Scandinavian journal of gastroenterology (2015). Not Altered. CC.
Antral mucosa. Normal (A): Normal number of antral G cells with typical “hallo” appearances occur in neck area of the pyloric glands (arrows). Non-atrophic chronic gastritis (B): Mononuclear inflammation occupies the whole mucosa giving an impression of gland loss (atrophy). Atrophic gastritis of mild to moderate degree in antrum (C): Inflammation is relative mild but there is a large area of pyloric glands lost and replaced with metaplastic glands (IM) as indicated with arrows. Severe atrophic gastritis in antrum (D): All pyloric glands are gone and the whole mucosa is “intestinalized”. Inflammation is mild, or moderate at most. Also the antral G cells are disappeared along with the loss of the normal pyloric glands. Therefore, the G-17 feedback response in physiological control of acid secretion is impaired. HE and Alcian blue – PAS stains × 300. Chronic gastritis. Sipponen P, Maaroos HI - Scandinavian journal of gastroenterology (2015). Not Altered. CC.


Peptic Ulcer Disease
Peptic ulcer disease is a mucosal ulcer of the gastrointestinal tract.
Peptic ulcer disease commonly involves the proximal duodenum (90 percent) or distal stomach (10 percent).
Causes of peptic ulcer diseases include:
- H. pylori is nearly often the cause of duodenal ulcers (> 95 percent)
- Zollinger Ellison (ZE) disease occasionally
- Non-steroidal anti-inflammatory (NSAID) medications
- Bile reflux
Peptic ulcer disease presents with epigastric pain that gets better with food.
Endoscopic diagnostic biopsies reveal Brunner gland hyperplasia and ulceration if the duodenum is involved.
Peptic ulcers may rupture, resulting in acute pancreatitis or anterior ulcer bleeding from the gastroduodenal artery (posterior ulcer).
The smaller curvature of the antrum is where an ulcer is most frequently found.
The left stomach artery may bleed during a rupture.
The majority of benign peptic ulcers are small (less than 3 cm), well defined, and encircled by radiating folds of mucosa.
Nearly seldom are duodenal ulcers cancerous (duodenal carcinoma is extremely rare).
Carcinoma is a differential diagnosis for peptic ulcers.
Gastric cancer can result in stomach peptic ulcers (intestinal subtype).
Malignant ulcers are big, asymmetrical, and have piled-up margins.
Biopsy is needed for definitive diagnosis.
 Peptic Ulcer Disease. Gastric ulcer. BruceBlaus - Not altered. CC BY-SA 4.0
Peptic Ulcer Disease. Gastric ulcer. BruceBlaus - Not altered. CC BY-SA 4.0






Gastric Carcinoma
Gastric carcinoma is the malignant proliferation of surface epithelial cells (adenocarcinoma) in the stomach.
Gastric carcinoma is sub-categorized as:
- Diffuse
- Intestinal forms
Laparoscopy of gastric carcinomas typically show a big, uneven ulcer with heaped-up edges characterizes the intestinal kind, which is more prevalent.
Gastric carcinoma typically affects the smaller curvature of the antrum (similar to gastric ulcer).
Risk factors for gastric carcinoma include:
- Intestinal metaplasia (from H. pylori and/or autoimmune gastritis)
- Consumption of nitrosamines in smoked foods (common in Japan)
Symptoms of gastric carcinoma include:
- Abdominal pain
- Fatigue
- Weight loss
- Early satiety
- Anemia
Metastasis of gastric carcinoma may affect the left supraclavicular node (Virchow node).
The liver is the site of distant metastasis of gastric carcinoma most frequently.
Intestinal gastric carcinoma commonly affects the periumbilical area (Sister Mary Joseph nodule).
Diffuse gastric carcinoma may involve the ovaries (Krukenberg tumor).
 Gastric Carcinoma. Adenocarcinoma of the stomach and intestinal metaplasia. H&E stain. Nephron - Not altered. CC BY-SA 3.0
Gastric Carcinoma. Adenocarcinoma of the stomach and intestinal metaplasia. H&E stain. Nephron - Not altered. CC BY-SA 3.0











