Bone Pathology
Achondroplasia
Achondroplasia literally means without chondrocyte growth.
A-chondro-plasia.
Achondroplasia is characterized by decreased cartilage proliferation in the development plate.
Achondroplasia is the most common cause of dwarfism.
Achondroplasia is related to an autosomal dominant (AD) activating mutation in fibroblast growth factor receptor 3 (FGFR3).
Overexpression of fibroblast growth factor receptor 3 (FGFR3) inhibits growth.
Most mutations of fibroblast growth factor receptor 3 (FGFR3) are sporadic and related to increased paternal age.
Because intramembranous bone production is unaffected, having short extremities with a normal-sized head and chest due to deficient endochondral bone formation is a clinical characteristic of achondroplasia.
The formation of an endochondral bone matrix is characterized by the formation of a cartilage matrix, which is eventually replaced by bone.
The formation of an endochondral bone matrix is the process by which long bones develop.
Intramembranous bone development, on the other hand, is distinguished by the production of bone without the presence of a preexisting cartilage matrix.
Intramembraneous bone formation is the process by which flat bones like the skull and rib cage form.
Mental function, life span, and fertility are not affected by achondroplasia.
 (a-d) AP radiographs of the lower limbs in achondroplasia (three boys and one girl of 6, 7, 8 and 9 years-old respectively), allmanifested the characteristic radiographic features of achondroplasia; shortness of the tubular long bones, with a relative increase in bonydiameters and densities are apparent. The metaphyses are widened and flared, but the epiphyses are uninvolved. The growth plates are U-shapedor V-shaped. This is best seen at the distal femur. The long bones, especially the tibiae, are bowed. The pelvis characteristicallyappears broad and flat, with squared iliac wings. The ilium appeared broad because the pelvis is formed almost entirely by intramemberanousossification, which is undisturbed in achondroplasia. The sciatic notches are small and the acetabuli are horizontal. Genu vara was a constantskeletal deformity encountered. In addition there was a relative shortening of the tibia compared to the fibular length. This tibial shortening istypically associated with a relevant ankle joint varus evolving during growth, the varus deformity ranged between 15 to 20°.Treatment of varus deformities of the lower limbs in patients with achondroplasia and hypochondroplasia. Kaissi AA, Farr S, Ganger R, Hofstaetter JG, Klaushofer K, Grill F - The open orthopaedics journal (2013). Not Altered. CC.
(a-d) AP radiographs of the lower limbs in achondroplasia (three boys and one girl of 6, 7, 8 and 9 years-old respectively), allmanifested the characteristic radiographic features of achondroplasia; shortness of the tubular long bones, with a relative increase in bonydiameters and densities are apparent. The metaphyses are widened and flared, but the epiphyses are uninvolved. The growth plates are U-shapedor V-shaped. This is best seen at the distal femur. The long bones, especially the tibiae, are bowed. The pelvis characteristicallyappears broad and flat, with squared iliac wings. The ilium appeared broad because the pelvis is formed almost entirely by intramemberanousossification, which is undisturbed in achondroplasia. The sciatic notches are small and the acetabuli are horizontal. Genu vara was a constantskeletal deformity encountered. In addition there was a relative shortening of the tibia compared to the fibular length. This tibial shortening istypically associated with a relevant ankle joint varus evolving during growth, the varus deformity ranged between 15 to 20°.Treatment of varus deformities of the lower limbs in patients with achondroplasia and hypochondroplasia. Kaissi AA, Farr S, Ganger R, Hofstaetter JG, Klaushofer K, Grill F - The open orthopaedics journal (2013). Not Altered. CC.
Osteogenesis Imperfecta (OI)
Osteogenesis imperfecta (OI) is a congenital bone resorption disease that results in structurally weak bone.
Osteogenesis imperfecta (OI) is caused by an autosomal dominant defect in collagen type I synthesis.
Clinical symptoms of osteogenesis imperfecta (OI) include:
- Blue sclera
- Hearing loss
- Multiple fractures of the bone
Note that the middle ear bones are also prone to fracture in osteogenesis imperfecta (OI).
Middle ear bones are also prone to fracture in osteogenesis imperfecta (OI).
 Osteogenesis Imperfecta. he classic blue sclera of a person with osteogenesis imperfecta Herbert L. Fred, MD and Hendrik A. van Dijk. Not altered. CC BY-SA 3.0
Osteogenesis Imperfecta. he classic blue sclera of a person with osteogenesis imperfecta Herbert L. Fred, MD and Hendrik A. van Dijk. Not altered. CC BY-SA 3.0







Osteopetrosis
Osteopetrosis is due to a hereditary deficiency in bone resorption.
Osteopetrosis causes abnormally thick, heavy bone that is brittle and easily fractures.
Multiple genetic variants exist, and carbonic anhydrase mutation leads to loss of the acidic microenvironment required for bone resorption.
Clinical features of osteopetrosis include:
- Bone fractures
- Anemia
- Thrombocytopenia
- Leukopenia
- Extramedullary hematopoiesis due to bony replacement of the marrow space
Impingement on cranial nerves due to bony overgrowth may cause characteristic neurologic symptoms based on the cranial nerves that are affected.
Osteopetrosis most often causes vision and hearing loss.
A carbonic anhydrase mutation causes renal tubular acidosis, while a lack of carbonic anhydrase causes poor HCO3 tubular reabsorption, which results in metabolic acidosis.
Treatment of osteopetrosis is bone marrow transplant since osteoclasts are derived from monocytes.
 Osteopetrosis. A 17-year-old male with osteopetrosis: Typical cranial deformity and thoracic scoliosis Konstantinos C Soultanis, Alexandros H Payatakes, Vasilios T Chouliaras, Georgios C Mandellos, Nikolaos E Pyrovolou, Fani M Pliarchopoulou and Panayotis N Soucacos. not altered. CC BY 2.0.
Osteopetrosis. A 17-year-old male with osteopetrosis: Typical cranial deformity and thoracic scoliosis Konstantinos C Soultanis, Alexandros H Payatakes, Vasilios T Chouliaras, Georgios C Mandellos, Nikolaos E Pyrovolou, Fani M Pliarchopoulou and Panayotis N Soucacos. not altered. CC BY 2.0.


Rickets
Rickets is defective mineralization of osteoid that effects children.
Osteomalacia is defective mineralization of osteoid that effects adults.
Both rickets and osteomalacia are related to vitamin D deficiency.
Vitamin D is crucial for bone health.
Osteoblasts normally produce osteoid, which is then mineralized with calcium and phosphate to form bone.
Low levels of vitamin D, can result in low serum calcium and phosphate.
In general:
- 85% of vitamin D is typically produced by the skin after exposure to sunlight
- 15% of vitamin D comes from diet
Activation of vitamin D requires 25-hydroxylation by the liver followed by alpha-hydroxylation by the proximal tubule cells of the kidney.
On the other hand, active vitamin D raises serum calcium and phosphate by acting on intestines and kidneys.
While the kidney enhances reabsorption of calcium and phosphate, the colon increases absorption of both substances.
Additionally, the bone promotes calcium and phosphate absorption.
Risk factors for vitamin D insufficiency included:
- Reduced sun exposure in northern latitudes
- Poor diet
- Malabsorption of fat-soluble vitamins
- Liver failure
- Renal failure
Low vitamin D levels in children cause improper bone mineralization, which causes rickets.
Common features of rickets include:
- Pigeon breast deformity
- Rachitic rosary chest
- Frontal bossing
- Large forehead
Rickets is pathognomonic associated with “pigeon-breast deformity” on chest X-ray
The pigeon chest deformity is the inward bending of the ribs with anterior protrusion of the sternum.
Rachitic rosary in children is caused by osteoid deposition at the costochondral junction.
Frontal bossing or having a larger forehead due to osteoid deposition on the skull is another common symptom of rickets in children.
Osteomalacia in adults is caused by inadequate vitamin D levels.
Inadequate mineralization results in weak bone with an increased risk for fracture.
Laboratory findings of rickets and osteomalacia include:
- Decreased serum calcium
- Decreased serum phosphate
- Increased parathyroid hormone (PTH)
- Increased alkaline phosphatase
 Rickets. Chest X-ray showing changes consistent with rickets. These changes are usually referred to as "rosary beads" of rickets. Frank Gaillard - Not altered. CC BY-SA 3.0
Rickets. Chest X-ray showing changes consistent with rickets. These changes are usually referred to as "rosary beads" of rickets. Frank Gaillard - Not altered. CC BY-SA 3.0




Osteoporosis
Osteoporosis is characterized by reduced trabecular bone mass, which leads to porous bone with a higher risk of fracture.
The peak bone mass reached in early adulthood and the following rate of bone loss are the two factors that determine osteoporosis risk.
By the age of 30-years-old, bone mass reaches its peak and is determined by hereditary factors, such as variations in the vitamin D receptor, diet, and exercise.
After peak bone mass is reached, approximately 1% of bone mass is lost annually.
The decrease in bone mass may be slowed by:
- Weight-bearing exercise
- Strength training
- Proper nutrition
Also note that estrogen is positively correlated with building and maintaining bone mass, thus once women stop producing estrogen they are at increased risk of osteoporosis.
The most common forms of osteoporosis are senile and postmenopausal.
Clinical symptoms of osteoporosis include:
- Hip pain
- Distal radius pain
- Fractures in weight-bearing vertebrae that cause kyphosis and height loss
- Bone pain
Bone density is measured using a dual X-ray absorptiometry (DEXA) scan.
In order to rule out osteomalacia, which has a similar clinical presentation to osteoporosis, the serum levels of calcium, phosphate, parathyroid hormone (PTH), and alkaline phosphatase are normal.
Treatment of osteoporosis includes:
- Exercise
- Vitamins
- Calcium
- Bisphosphonates
Bisphosphonates are a type of medicine that promotes apoptosis of osteoclasts.
Contrarily, the use of estrogen replacement treatment is debatable and not currently advised.
The use of glucocorticoids is contraindicated because it may worsen osteoporosis.
 Osteoporosis. Multiple osteoporotic wedge fractures demonstrated on a lateral thoraco-lumbar spine X-ray Glitzy queen00. Not altered. Public Domain.
Osteoporosis. Multiple osteoporotic wedge fractures demonstrated on a lateral thoraco-lumbar spine X-ray Glitzy queen00. Not altered. Public Domain.





Paget Disease of the Bone
Paget disease of the bone is due to the imbalance between osteoclast and osteoblast function.
Paget disease of the bone often manifests in late adulthood with an average age of more than 60-years-old.
The cause of Paget disease of the bone is unknown, but it might be viral.
One or more bones are involved in a localized process that does not affect the entire skeleton.
There are three stages of Paget disease of the bone which include:
- Osteoclastic
- Mixed osteoblastic-osteoclastic
- Osteoblastic
The end consequence of Paget disease of the bone is bone that is dense, sclerotic, and brittle.
Histology of Paget disease of the bone reveals a mosaic pattern of lamellar bone.
Clinical signs of Paget disease of the bone include:
- Hearing loss
- Enlarging head size (having to obtain bigger hats)
- Bone pain
- Microfractures
Patients older than 40-years-old are more likely to have isolated increased alkaline phosphatase, which is the most prevalent cause of isolated raised alkaline phosphatase.
Patients with Paget disease of the bone also tend to have lion-like facies with involvement of the craniofacial bones.
Treatment of Paget disease of the bone includes:
- Calcitonin
- Bisphosphonates
Calcitonin inhibits osteoclast function.
Bisphosphonates induce apoptosis of osteoclasts.
Complications of Paget disease of the bone include:
- Osteosarcoma
- High output heart failure
 Paget Disease of the Bone. Paget's disease of right innominate bone. Man of 80 years age. Jmarchn - Not altered. CC BY-SA 3.0
Paget Disease of the Bone. Paget's disease of right innominate bone. Man of 80 years age. Jmarchn - Not altered. CC BY-SA 3.0




Osteomyelitis
Osteomyelitis is an infection of bone.
Osteomyelitis is most commonly caused by bacteria, and arises via hematogenous spread.
While open-wound bacteremia in adults typically seeds epiphysis, transient bacteremia in infants usually seeds the metaphysis.
Staphylococcus aureus is the most common cause of osteomyelitis, accounting for 90% of cases.
Common causes of osteomyelitis include:
- Staphylococcus aureus (90% of cases)
- Neisseria gonorrhoeae which affects sexually active young adults
- Salmonella
- Pseudomonas in diabetics and drug users
- Pasteurella, which is linked to cat and dog bites and scratches
- Mycobacterium tuberculosis, which typically affects the vertebrae
Clinical characteristics of osteomyelitis include:
- Bone pain
- Signs of systemic infection symptoms
- X-ray showing a lytic center surrounded by bone sclerosis
Lytic focus is called sequestrum, and sclerosis is called involucrum.
Diagnosis of osteomyelitis is made by blood culture and/or bone biopsy at the site of the lesion.
 Osteomyelitis. Osteomyelitis in both feet as seen on bone scan James Heilman, MD - Not altered, CC BY-SA 4.0
Osteomyelitis. Osteomyelitis in both feet as seen on bone scan James Heilman, MD - Not altered, CC BY-SA 4.0





Avascular Necrosis
Avascular necrosis is an ischemic necrosis of bone and bone marrow caused by trauma or fracture.
Risk factors for avascular necrosis include:
- Steroid use
- Sickle cell anemia
- Caisson disease (acute decompression syndrome deep sea divers may experience)
Complications of avascular necrosis include:
- Osteoarthritis
- Fractures
 Avascular Necrosis. Pathology of avascular necrosis, with a photograph of a cross-section of the involved bone at top left. The reactive zone shows irregular trebaculae with empty lacunae, and fibrosis of the marrow space. Mikael Häggström, M.D. Not altered. CC0.
Avascular Necrosis. Pathology of avascular necrosis, with a photograph of a cross-section of the involved bone at top left. The reactive zone shows irregular trebaculae with empty lacunae, and fibrosis of the marrow space. Mikael Häggström, M.D. Not altered. CC0.






Bone Tumors
Osteoma
Osteoma is a benign tumor of the bone.
Osteoma most commonly arises on the surface of facial bones.
Osteomas are associated with Gardner syndrome.
 Osteoma. Osteoma James Heilman, MD - Not altered. CC BY-SA 4.0
Osteoma. Osteoma James Heilman, MD - Not altered. CC BY-SA 4.0



Osteoid Osteoma
Osteoid osteoma is a subtype of osteoma.
In osteoid osteoma, reactive bone forms a ring around a benign tumor of osteoblasts, which produce osteoid.
Osteoid osteoma occurs more commonly in young adults (younger than 25 years of age), and is more common in males.
When osteoid osteoma develops in the cortex of a long bone, such as the femur, it causes bone discomfort that can be managed with aspirin.
Imaging of osteoid osteoma classically reveals a bony mass (< 2.0 cm) with a radiolucent core (osteoid).
The main differential to osteoid osteoma is an osteoblastoma.
Osteoblastomas are similar to osteoid osteomas, however osteoblastomas are larger bigger (> 2.0 cm), may develop in the vertebrae, and manifests as bone pain that is not relieved by aspirin.
 Osteoid Osteoma. CT scan showing an osteoid osteoma of the fibula with a clearly visible nidus Hellerhoff -Not altered. CC BY-SA 3.0
Osteoid Osteoma. CT scan showing an osteoid osteoma of the fibula with a clearly visible nidus Hellerhoff -Not altered. CC BY-SA 3.0



Osteochondroma
Osteochondroma is the tumor of bone with an overlying cartilage cap.
Osteochondroma is the most common type of benign tumor of bone.
Since the bone and marrow space are one continuous structure, the tumor is the result of the growth plate projecting laterally.
Overlying cartilage can transform into chondrosarcoma on rare occasions.
 Osteochondroma. Surgical extraction of osteochondromas is sometimes beneficial. Shown is an osteochondroma surgically extracted from a ten-year-old patient. The bone is the cylindrical stalk at the bottom, about 1/2 inch long, the two diagonal growths are cartilage. This morphology is typical of a tibial bone spur. - Not altered.. CC BY-SA 3.0
Osteochondroma. Surgical extraction of osteochondromas is sometimes beneficial. Shown is an osteochondroma surgically extracted from a ten-year-old patient. The bone is the cylindrical stalk at the bottom, about 1/2 inch long, the two diagonal growths are cartilage. This morphology is typical of a tibial bone spur. - Not altered.. CC BY-SA 3.0

Osteosarcoma
Osteosarcoma is the malignant proliferation of osteoblasts.
Osteosarcomas typically develop in the metaphysis of long bones, i.e. the proximal tibia or distal femur.
Risk factors for osteosarcoma include:
- Familial retinoblastoma
- Paget disease
- Radiation exposure
Peak incidence of osteosarcoma is seen in teenagers and less commonly seen in the elderly.
Osteosarcoma typically presents as a pathologic fracture or bone pain with swelling.
Radiology of osteosarcoma classically shows a destructive mass with a “sunburst” appearance, and elevation of the periosteum.
Diagnosis of osteosarcoma is made by biopsy, which will show pleomorphic cells that create osteoid.
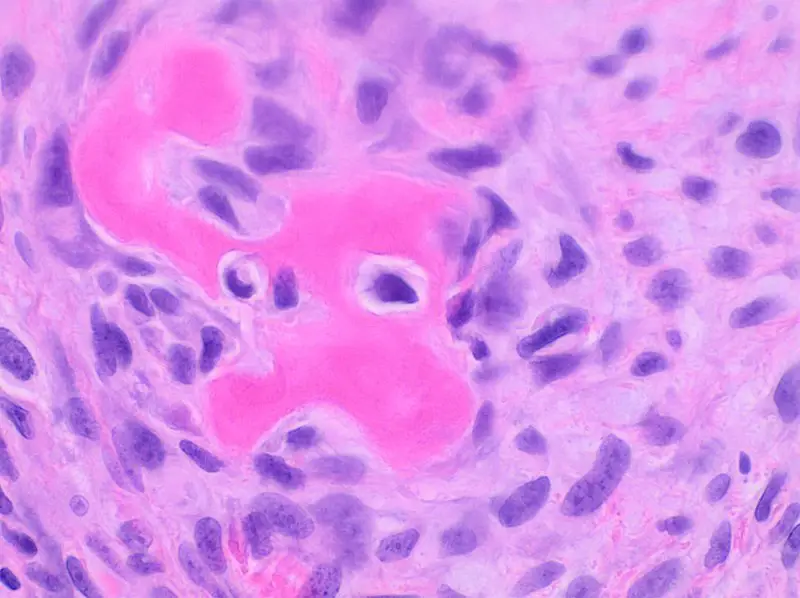
 Osteosarcoma. Intermediate magnification micrograph of a high-grade osteosarcoma. H&E stain. By definition, osteosarcomas form osteoid (the organic extracellular component of bone), which is pink, bland/homogenous on H&E staining. Related images Low mag. Intermed. mag. High mag. Very high mag. Nephron -Not altered CC BY-SA 3.0
Osteosarcoma. Intermediate magnification micrograph of a high-grade osteosarcoma. H&E stain. By definition, osteosarcomas form osteoid (the organic extracellular component of bone), which is pink, bland/homogenous on H&E staining. Related images Low mag. Intermed. mag. High mag. Very high mag. Nephron -Not altered CC BY-SA 3.0



Giant Cell Tumor of the Bone
Giant cell tumor of the bone is composed of multinucleated giant cells and stromal cells that occur in young adults.
Giant cell tumor of the bone typically arises in the epiphysis of long bones, usually the distal femur or proximal tibia.
Radiology of giant cell tumor of the bone classically shows a “soap-bubble” appearance on x-ray.
Giant cell tumors of the bone are locally aggressive, and they may recur after surgical removal.
 Giant Cell Tumor of the Bone. X-ray of a giant-cell bone tumor in the head of the fourth metacarpal of the left hand James Heilman, MD. Not altered. Public Domain.
Giant Cell Tumor of the Bone. X-ray of a giant-cell bone tumor in the head of the fourth metacarpal of the left hand James Heilman, MD. Not altered. Public Domain.



Ewing Sarcoma
Ewing sarcoma is characterized by the malignant proliferation of poorly differentiated cells.
Ewing sarcoma typically affects male children under the age of 15-years-old.
Ewing sarcoma generally manifests in the diaphysis of the long bones.
Radiology of Ewing sarcoma classically has an “onion-skin” appearance on X-ray.
Diagnosis of Ewing sarcoma is made by biopsy that reveals small, round, blue cells that look similar to lymphocytes.
Malignant cells of Ewing sarcoma stain positive for CD99.
Genetic tests for Ewing sarcoma tend to show EWSR translocations, such as EWSR-FLI1.
Ewing sarcoma is treated by chemotherapy.
 Ewing Sarcoma. Magnetic resonance imaging slice showing Ewing sarcoma of the left hip (white area shown right) Unknown photographer/artist - National Cancer Institute, AV Number: AV-0000-4364. Not altered. Public Domain
Ewing Sarcoma. Magnetic resonance imaging slice showing Ewing sarcoma of the left hip (white area shown right) Unknown photographer/artist - National Cancer Institute, AV Number: AV-0000-4364. Not altered. Public Domain






Chondroma
Chondromas are benign tumors composed of cartilage.
Chondromas typically develops in the medulla of the small bones in the hands and feet.
 Chondroma. Lantern slide: Multiple Chondromata of fingers. Not altered. CC-BY-4.0
Chondroma. Lantern slide: Multiple Chondromata of fingers. Not altered. CC-BY-4.0
Chondrosarcoma
Chondrosarcoma is a malignant cartilage-forming tumor.
Chondrosarcomas tend to develop in the axial skeleton or pelvic medulla.
Diagnosis of chondrosarcoma is made by biopsy, which shows malignant chondrocytes.
 Chondrosarcoma. Histopathogic image of chodrosarcoma of the chest wall. Surgical resection of recurrent mass. H & E stain. No machine-readable author provided. KGH assumed (based on copyright claims). - No machine-readable source provided. Own work assumed (based on copyright claims). Not altered. CC BY-SA 3.0
Chondrosarcoma. Histopathogic image of chodrosarcoma of the chest wall. Surgical resection of recurrent mass. H & E stain. No machine-readable author provided. KGH assumed (based on copyright claims). - No machine-readable source provided. Own work assumed (based on copyright claims). Not altered. CC BY-SA 3.0



Metastatic Tumors to the Bone
Primary cancers are less frequent than metastatic tumors to the bone.
Metastatic tumors to the bone typically show osteolytic, punched-out lesions on X-ray.
Notably, metastatic prostate cancer to the bone produces osteoblastic lesions.

