Demyelinating Disorders Pathology Video
Demyelinating Disorders
Demyelinating disorders are pathologic conditions due to the degeneration of myelin.
Axons are insulated by myelin, which increases conduction efficiency and speed.
Oligodendrocytes myelinate the central nervous system.
Schwann cells myelinate the peripheral nervous system.
Myelin and oligodendrocytes are typically destroyed in demyelinating illnesses, but axons are typically retained.
Examples of demyelinating disorders include:
- Leukodystrophies
- Multiple sclerosis
- Subacute sclerosing panencephalitis
- Progressive multifocal leukodystrophy (PML)
- Central pontine myelinolysis
Leukodystrophies
Leukodystrophies are due to mutations that are inherited in the myelin-producing or myelin-maintaining enzymes.
The most prevalent form of leukodystrophy, metachromatic leukodystrophy, is caused by an autosomal recessive arylsulfatase deficiency.
Metachromatic leukodystrophy
In metachromatic leukodystrophy, arylsulfatase deficiency results in myelin build up in oligodendrocyte lysosomes because it cannot be broken down (lysosomal storage disease).
Krabbe disease
Galactocerebroside p-galactosidase deficiency causes Krabbe disease in an autosomal recessive pattern.
Macrophages accumulate galactocerebroside in Krabbe disease.
Adrenaleukodystrophy
Adrenoleukodystrophy is caused by an X-linked mutation.
Adrenoleukodystrophy causes the addition of coenzyme A to long-chain fatty acids to be hindered.
In adrenoleukodystrophy, fatty acid buildup harms the brain’s white matter and glands.
 Leukodystrophies. Globoid cell leukodystrophy PAS - Multinucleated macrophages ("globoid cells") and loss of myelinated fibers in a case of Krabbe's leukodystrophy Jensflorian - Not altered. CC BY-SA 3.0
Leukodystrophies. Globoid cell leukodystrophy PAS - Multinucleated macrophages ("globoid cells") and loss of myelinated fibers in a case of Krabbe's leukodystrophy Jensflorian - Not altered. CC BY-SA 3.0



Multiple Sclerosis (MS)
Multiple sclerosis (MS) is the most common chronic central nervous system (CNS) disease of young adults (20 – 30 years of age), and is more frequently found in women.
Multiple sclerosis (MS) results from autoimmune myelin and oligodendrocyte destruction.
Multiple sclerosis (MS) is associated with HLA-DR2.
Multiple sclerosis (MS) is observed more frequently in areas further from the equator.
Multiple sclerosis (MS) is associated with recurrent neurologic impairments with times of remission are present (multiple lesions in time and space).
Clinical symptoms of multiple sclerosis (MS) include:
- Blurry vision (optic nerve(s))
- Vertigo and scanning speech that resemble alcohol intoxication (brainstem)
- Internuclear ophthalmoplegia (medial longitudinal fasciculus)
- Hemiparesis is a loss of sensation to one side (cerebral white matter, usually periventricular)
- Weakness or lack of feeling in the lower extremity (spinal cord)
- Malfunction of the bowels, bladder, and sexual (autonomic nervous system)
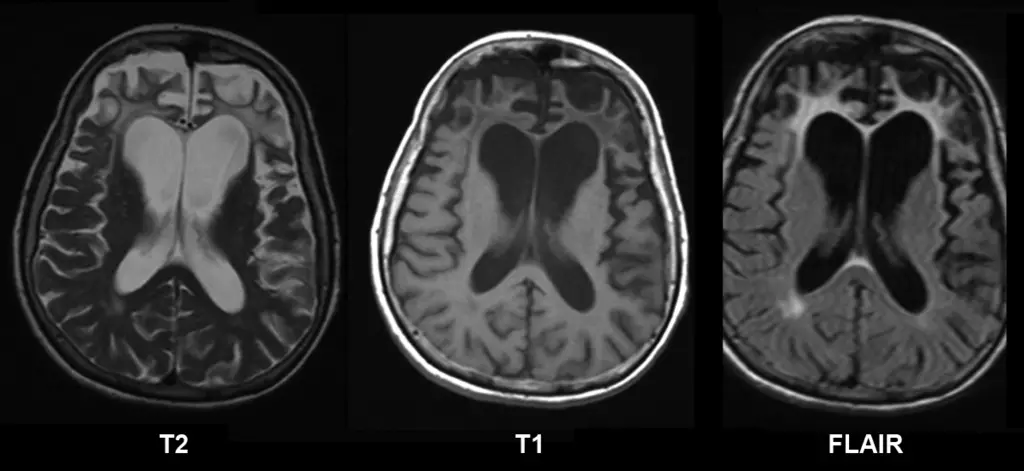
Both magnetic resonance imaging (MRI) and lumbar puncture (LP) are used to diagnose multiple sclerosis (MS).
Magnetic resonance imaging (MRI) identifies plaques (areas of white matter demyelination) associated with multiple sclerosis (MS).
Lumbar puncture findings of multiple sclerosis (MS) show:
- Increased oligoclonal bands
- Increased lymphocytes
- Myelin basic protein
Treatment of multiple sclerosis (MS) depends on the severity or timing of the attack:
- High-dose steroids are used in the treatment of acute attacks
- Interferon beta therapy for a long period of time reduces the disease’s progression.
Gross inspection of brains with multiple sclerosis (MS) reveal white matter plaques that appear gray.
 Multiple Sclerosis
Multiple Sclerosis




Subacute Sclerosing Panencephalitis
Subacute sclerosing panencephalitis is a progressive, fatal encephalitis that worsens over time.
Subacute sclerosing panencephalitis is due to the measles virus’s lingering, slowly spreading infection of the brain.
Measles infection starts in utero.
Neurologic symptoms associated with measles infection manifest in childhood.
Subacute sclerosing panencephalitis is characterized by viral inclusions in oligodendrocytes and gray matter neurons (white matter).
 Subacute Sclerosing Panencephalitis. Subacute sclerosing panencephalitis. Figure 1. MRI scans of the brain at the time of presentation in the neurology clinic (A and B) and 3 months later (C and D). Panels A and C are T1-weighted images; B and D are T2-weighted images. The initial MRI scan (A and B) reveals a focal abnormality in the subcortical white matter of the left frontal lobe, consisting of a hypointense signal on the T1-weighted image (arrow in A) and a hyperintense signal on the T2-weighted image (arrow in B). In the followup scan, the focal abnormality in the left frontal lobe is less obvious than previously (arrow in D), but advanced and diffuse cortical atrophy is present, signified by the ventriculomegaly and markedly enlarged sulci (arrowheads in C). Bonthius D, Stanek N, Grose C/ CDC - Bonthius D, Stanek N, Grose. Not altered. Public Domain
Subacute Sclerosing Panencephalitis. Subacute sclerosing panencephalitis. Figure 1. MRI scans of the brain at the time of presentation in the neurology clinic (A and B) and 3 months later (C and D). Panels A and C are T1-weighted images; B and D are T2-weighted images. The initial MRI scan (A and B) reveals a focal abnormality in the subcortical white matter of the left frontal lobe, consisting of a hypointense signal on the T1-weighted image (arrow in A) and a hyperintense signal on the T2-weighted image (arrow in B). In the followup scan, the focal abnormality in the left frontal lobe is less obvious than previously (arrow in D), but advanced and diffuse cortical atrophy is present, signified by the ventriculomegaly and markedly enlarged sulci (arrowheads in C). Bonthius D, Stanek N, Grose C/ CDC - Bonthius D, Stanek N, Grose. Not altered. Public Domain
Progressive Multifocal Leukoencephalopathy (PML)
Progressive multifocal leukodystrophy (PML) is caused by John Cunningham (JC) virus infection of oligodendrocytes (white matter).
John Cunningham (JC) virus is also known as human polyoma virus 2.
The latent JC virus is reactivated by immune suppression, such as:
- HIV infection
- AIDS
- Leukemia
- Immunosuppression status post (s/p) organ transplant
In progressive multifocal leukodystrophy (PML), rapid progression of neurologic symptoms (such as dementia, paralysis, and vision loss) eventually cause death.
 Progressive Multifocal Leukoencephalopathy. Progressive multifocal leukoencephalopathy (PML). Not altered. CC BY 3.0
Progressive Multifocal Leukoencephalopathy. Progressive multifocal leukoencephalopathy (PML). Not altered. CC BY 3.0
Central Pontine Myelinolysis
Central pontine myelinolysis is focal demyelination of the pons (anterior brain stem) due to rapid intravenous hyponatremia correction.
Risk factors for central pontine myelinolysis include:
- Liver disease
- Alcoholism
Locked in syndrome is the result of central pontine myelinolysis.
Locked in syndrome is characterized by acute bilateral paralysis.
 Central Pontine Myelinolysis. Axial fat saturated T2-Weighted MRI showing hyperintense signal in the central pons. The patient was an alcoholic admitted with a serum Na 101 who was treated with hypertonic saline. He had severe quadriparesis, and dysarthria. - Not altered. CC BY-SA 3.0
Central Pontine Myelinolysis. Axial fat saturated T2-Weighted MRI showing hyperintense signal in the central pons. The patient was an alcoholic admitted with a serum Na 101 who was treated with hypertonic saline. He had severe quadriparesis, and dysarthria. - Not altered. CC BY-SA 3.0

