Respiratory Distress Syndrome Pathology Video
Acute Respiratory Distress Syndrome
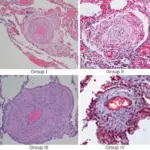
Acute respiratory distress syndrome (ARDS) is due to damage to the alveolar-capillary junction that is widespread (diffuse alveolar damage).
Edema and the development of hyaline membranes in alveoli are caused by the leakage of protein-rich fluid.
Clinical features of acute respiratory distress syndrome (ARDS) include:
- Respiratory distress
- Cyanosis
- Hypoxia
Air sacs collapse and a barrier (increased surface tension).
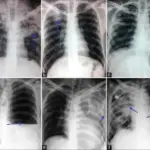
Chest x-ray classically shows “white-out” appearance in acute respiratory distress syndrome (ARDS).
Common causes of acute respiratory distress syndrome (ARDS) include:
- Medications
- Sepsis
- Infection
- Shock
- Trauma
- Aspiration
- Pancreatitis
- Disseminated intravascular coagulation (DIC)
- Hypersensitivity reactions
Type I and type II pneumocytes are damaged by protease-mediated and free radical reactions brought on by neutrophil activation.
Treatment of acute respiratory distress syndrome (ARDS) must address the root cause.
Positive end-expiratory pressure ventilation (PEEP) may be useful in supporting patients with acute respiratory distress syndrome.
Interstitial fibrosis can make recovery more difficult because it causes scarring and fibrosis when type pneumocytes are damaged or lost.
 Acute Respiratory Distress Syndrome. Severe ARDS. Person is intubated with an OG in place. James Heilman, MD - Not altered. CC BY-SA 4.0
Acute Respiratory Distress Syndrome. Severe ARDS. Person is intubated with an OG in place. James Heilman, MD - Not altered. CC BY-SA 4.0


Neonatal Respiratory Distress Syndrome
Neonatal respiratory distress syndrome is respiratory distress brought on by low levels of surfactant.
Type II pneumocytes produce surfactant, the main component of which is phosphatidylcholine (lecithin).
The lung’s surface tension is reduced by surfactant, limiting the collapse of the alveolar air sacs during expiration.
Lack of surfactant causes air sacs to burst and hyaline membranes to develop.
Neonatal respiratory distress syndrome is related to prematurity.
At 28 weeks gestation, surfactant production starts, but it takes until 34 weeks for appropriate amounts to be established.
Lung maturity is assessed using the lecithin to sphingomyelin ratio (L/S) of amniotic fluid.
As surfactant is created, phosphatidylcholine (lecithin) levels rise while sphingomyelin levels stay the same.
- A ratio of lecithin to sphingomyelin ratio of equal to or greater than 2:1 denotes sufficient surfactant production
- A ratio of lecithin to sphingomyelin ratio of less than 2:1 denotes risk
Lack of stress-induced hormones, which promote surfactant synthesis, led to cesarean deliveries.
Insulin reduces the formation of surfactants in maternal diabetes.
Clinical features of neonatal respiratory distress syndrome include:
- Grunting
- Tachypnea
- Auxiliary muscle usage
- Hypoxemia
- Cyanosis
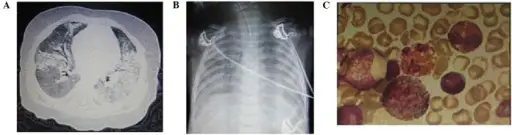
On X-ray, the lung’s diffuse granularity (or “ground-glass appearance”).
Complications include of neonatal respiratory distress syndrome:
- Necrotizing enterocolitis
- Blindness
- Bronchopulmonary dysplasia
The probability of necrotizing enterocolitis (NEC) and patent ductus arteriosus (PDA) persisting is increased by hypoxemia.
The likelihood of free radical damage is increased by additional oxygen.
Blindness results from retinal damage.
Bronchopulmonary dysplasia results from lung damage.
 Infant Respiratory Distress Syndrome. Chest radiograph one day after birth of a boy after 29 weeks and 3 days of gestational age who developed respiratory distress. It shows signs of infant respiratory distress syndrome (IRDS), in the form of a generalized fine granular opacities that creates air bronchograms. The thorax is bell-shaped due to decreased lung volume. In addition, there are both arterial and venous umbilical lines, a nasogastric tube and electrocardiography electrodes. Mikael Häggström, M.D. Not Altered. CC0.
Infant Respiratory Distress Syndrome. Chest radiograph one day after birth of a boy after 29 weeks and 3 days of gestational age who developed respiratory distress. It shows signs of infant respiratory distress syndrome (IRDS), in the form of a generalized fine granular opacities that creates air bronchograms. The thorax is bell-shaped due to decreased lung volume. In addition, there are both arterial and venous umbilical lines, a nasogastric tube and electrocardiography electrodes. Mikael Häggström, M.D. Not Altered. CC0.